
Disorganized attachment—also called fearful-avoidant attachment—is a pattern where a person simultaneously craves and fears closeness because the attachment figure was both the source of safety and the source of threat. Approximately 15 percent of non-clinical adults carry an unresolved/disorganized classification on the Adult Attachment Interview (Bakermans-Kranenburg and van IJzendoorn, 2009), rising to roughly 76 percent in clinical populations (AAI meta-analysis).
Unlike anxious or avoidant attachment, which rely on a single dominant strategy, disorganized attachment involves contradictory impulses firing at the same time—making standard therapy approaches insufficient. This article provides an evidence-tiered guide to the therapies that address the unique neurobiological and relational complexity of disorganized attachment, so you can make informed decisions about your healing. For whether healing is possible, see our companion article on whether disorganized attachment can be healed.
Key takeaway: EMDR is the only therapy with published evidence of shifting disorganized attachment to earned secure, measured by the Adult Attachment Interview. Effective treatment follows a phase-based model of stabilization, trauma processing, and integration, typically spanning one to two or more years. Body-based therapies like Sensorimotor Psychotherapy and IFS address the fragmented inner experience that makes disorganized attachment uniquely complex.
Why Does Disorganized Attachment Need a Different Therapeutic Approach?
Disorganized attachment requires specialized treatment because the therapeutic relationship itself triggers the wound. When your original caregiver was both safe haven and source of danger, your nervous system learned that closeness equals threat—and a therapist is, by definition, someone you're asked to get close to.
Main and Hesse (1990) described this as "fright without solution": the child needed to approach the very person who frightened them. That paradox doesn't disappear in adulthood. It shows up every time you sit across from a therapist and feel the simultaneous pull to trust and the urge to bolt.
Standard talk therapy and generic CBT often miss this because they assume a client can form a stable working alliance from the start. With disorganized attachment, the alliance is the work. Your nervous system carries contradictory internal working models—one that says "people are safety" and another that says "people are danger"—and both activate at once.
This simultaneous activation is what Porges describes as the "fear without solution" state: sympathetic arousal (fight/flight) and dorsal vagal shutdown (freeze/collapse) firing together. Roughly 76 percent of people in clinical treatment carry an unresolved/disorganized classification (AAI meta-analysis), suggesting that many people in therapy have this pattern—yet few therapies are designed specifically for it.
The Contradiction Inventory (for disorganized attachment)
- Write down 3 relationships where you feel pulled toward someone and simultaneously want to flee
- For each one, note what draws you in
- Note what makes you want to escape
- Locate where you feel each impulse in your body—the pull might live in your chest, the recoil in your shoulders or gut
- Read what you wrote without trying to resolve the contradiction
Externalizing the opposing impulses keeps them from controlling your behavior from the inside. For disorganized attachment, simply naming the contradiction begins to create "dual awareness"—the capacity to observe the pattern rather than be consumed by it, which is the foundation that therapy builds on.
Which Therapies Have the Strongest Evidence for Disorganized Attachment?
If you have searched for the right therapy and felt overwhelmed by contradictory advice, that confusion reflects how under-discussed this topic remains. EMDR is the only modality with published AAI-measured attachment change in adults with disorganized attachment. Beyond EMDR, therapies fall into an evidence-tiered hierarchy based on research strength—a distinction most guides fail to make.
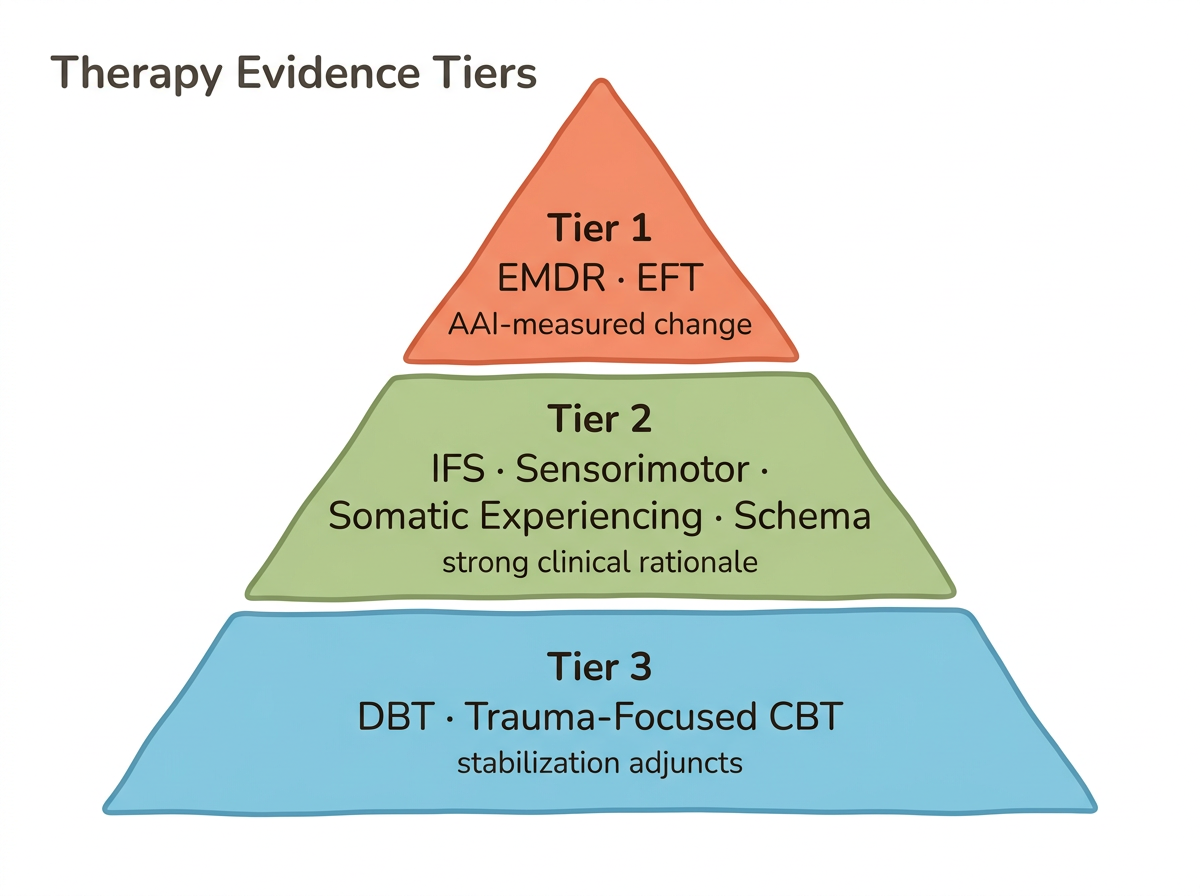
Tier 1: Published Attachment-Change Evidence
EMDR and Attachment-Focused EMDR stand alone in this tier. Wesselmann and Potter (2009) documented three adults shifting from insecure/disorganized to earned secure attachment after 10–15 sessions over approximately one year, measured by the AAI. Scelles and Bherer (2022) further supported EMDR's role in changing attachment state of mind. For couples, Emotionally Focused Therapy has the strongest RCT base—Johnson's research shows 77 percent of couples complete treatment successfully and 90 percent show significant improvement.
Tier 2: Strong Clinical Rationale, Emerging Evidence
The fragmented self-experience of disorganized attachment—where contradictory impulses coexist—finds a natural therapeutic match in Internal Family Systems, whose parts framework maps directly onto those opposing forces. Research on the "Inner Loving Parent" concept shows IFS moderates closeness terror. Sensorimotor Psychotherapy (Ogden and Fisher, 2015) and Somatic Experiencing work at the body level, where defensive responses remain incomplete: Sensorimotor Psychotherapy targets frozen action sequences while Somatic Experiencing addresses the oscillation between hyperarousal and shutdown. Schema Therapy rounds out this tier by targeting early maladaptive schemas in the disconnection/rejection domain.
Tier 3: Useful Adjuncts
DBT provides distress tolerance and emotion regulation skills essential for stabilization—particularly helpful when disorganized attachment co-occurs with borderline features. Trauma-focused CBT offers cognitive restructuring of fear-based internal working models.
For a broader look at how therapy can change attachment style, see our general overview.
Therapy Readiness Self-Check (for disorganized attachment)
- Rate your distress tolerance on a scale of 1–10. Can you sit with difficult emotions for 60 seconds without dissociating or acting on impulse?
- When emotions arise, can you name them—or do you mostly feel numb, then suddenly overwhelmed?
- Have you maintained a stable therapeutic relationship for at least 3 months before?
- Check for co-occurring patterns: dissociation, self-harm, substance use, chronic emptiness
A low score here is not a failing—it reflects how much your nervous system is still protecting you. It simply means stabilization work comes first. If you scored below 4 on distress tolerance, struggle to name emotions, or have active co-occurring symptoms, stabilization-focused work (Tier 3 adjuncts like DBT skills) should come before trauma processing. If you can stay present with discomfort and have some therapeutic relationship experience, Tier 1 and 2 modalities may be appropriate. For disorganized attachment, the tendency to oscillate between "I'm fine" and "I'm falling apart" makes honest self-assessment difficult—this check helps you gauge actual nervous system readiness rather than relying on willpower alone.
How Does EMDR Rewire Disorganized Attachment Patterns?
EMDR rewires disorganized attachment by reprocessing the traumatic memories that created the pattern—without requiring the verbal narrative that disorganized clients often cannot access due to dissociative lapses in discourse.
Bilateral stimulation—alternating left-right sensory input through eye movements, tapping, or auditory tones—appears to reduce the emotional charge of traumatic memories while the brain reconsolidates them. For disorganized attachment, this matters because the core memories involve a paradox: reaching toward a caregiver who was simultaneously frightening. Those memories often live below language, stored as body sensations, fragmented images, and contradictory impulses.
Attachment-Focused EMDR, developed by Laurel Parnell (2008), takes standard EMDR further. Where traditional EMDR starts with a specific traumatic memory, AF-EMDR begins by building internal attachment resources—imagined nurturing figures, safe places, protector figures—before processing relational trauma. This is critical for disorganized attachment because these individuals often lack any internalized template for safety.
Wesselmann and Potter's (2009) case studies reveal the process in detail. One client began treatment with a Dismissive plus Unresolved/disorganized classification on the AAI. After approximately one year of sessions, they tested as earned secure. The key mechanism was building dual awareness—the ability to hold the traumatic memory and present-moment safety simultaneously, which is precisely what disorganized attachment prevents.
Butterfly Hug Resource Installation (somatic/body-based, for disorganized attachment)
- Cross your arms over your chest, placing each hand on the opposite shoulder
- Begin alternating taps—left, right, left, right—slowly, about one tap per second
- While tapping, bring to mind one moment you felt genuinely safe with another person. Even a brief moment counts
- Notice where that safety registers in your body—warmth in your chest, softness in your jaw, release in your shoulders
- If fear arises alongside the safety feeling, that is the disorganized pattern showing up. Do not push it away. Simply notice that both exist at the same time
- Continue tapping for 30–60 seconds, holding both experiences
Over time, your nervous system learns that safety and connection can coexist—an experience your early environment may never have provided. For disorganized attachment specifically, this dual awareness capacity is what EMDR relies on, and even brief practice outside sessions strengthens it.
What Does the Phase-Based Treatment Model Look Like?
Phase-based treatment is the clinical gold standard for disorganized attachment, moving through three stages: stabilization, trauma processing, and integration. Skipping Phase 1 is the most common clinical error with disorganized clients—and the fastest route to therapy dropout.
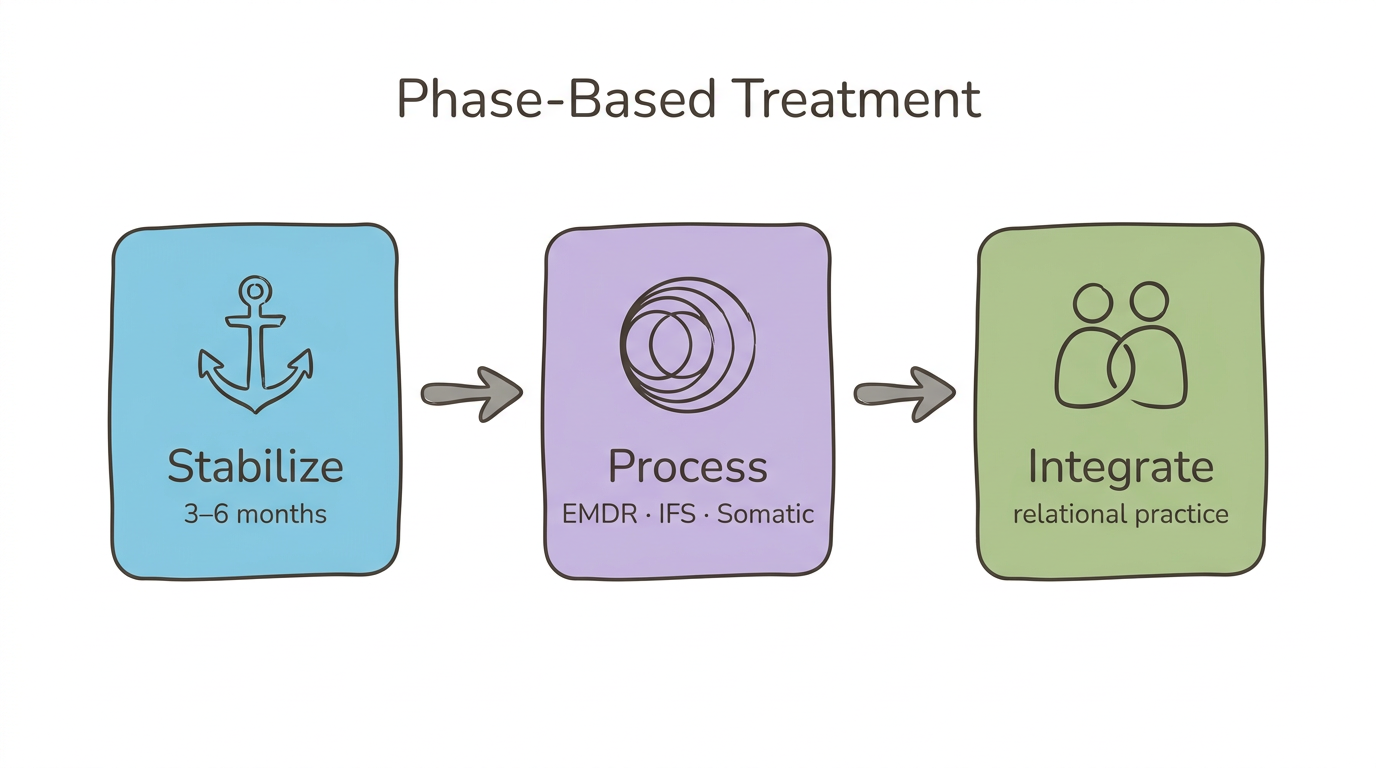
Phase 1: Stabilization and Safety
Your nervous system learned that connection equals danger. Before any trauma processing can begin, you need a foundation of distress tolerance and a therapeutic relationship that feels predictable. This phase involves grounding skills, emotion identification, and learning to recognize your window of tolerance. DBT skills are particularly useful here. This phase may last 3–6 months or longer.
Phase 2: Trauma Processing
Once stabilization is established, modalities like EMDR, IFS parts work, and sensorimotor processing can address the frozen defensive responses that sustain the disorganized pattern. Your therapist helps you reprocess the specific memories and body experiences where approach and avoidance became fused.
Phase 3: Integration and Relational Skills
The final phase consolidates earned security—practicing new relational behaviors, testing vulnerability in safe relationships, and building the internal working model your childhood didn't provide. Couples work through EFT can enter here. Herman (1992) originally described this phase-based framework for complex trauma, and it remains the cornerstone of disorganized attachment treatment. Ogden and Fisher (2015) extended it to include body-level processing at each phase.
Treatment typically spans 1–2 or more years. Your healing will not be linear, and that is expected.
Phase Mapping Journal (for disorganized attachment)
- Each evening for one week, answer three questions in writing
- Phase 1 check: "Did I feel safe enough to notice my emotions today?" Record yes, no, or partly
- Phase 2 check: "Did a memory or body sensation surface that felt connected to old relationships?"
- Phase 3 check: "Did I practice a new relational behavior—asking for help, setting a boundary, staying present during conflict?"
- After 7 days, notice which phase has the most entries
The phase with the most activity reflects where your nervous system is currently working. Disorganized attachment often keeps people bouncing between phases—one day you feel stable, the next a trigger sends you back to survival mode. This journal helps you and your therapist track your actual phase rather than assuming a linear trajectory.
Why Do Body-Based Therapies Matter for Disorganized Attachment?
Body-based therapies matter because disorganized attachment is stored as incomplete defensive responses in the body—not just as thoughts or beliefs. Neuroscience confirms that this pattern produces measurable changes in brain structure and autonomic function that talk therapy alone cannot reach.
Research by Noce and colleagues (2023) found that disorganized attachment in infancy predicts an enlarged amygdala volume by adulthood, with the left amygdala specifically associated with dissociation and limbic irritability. An fMRI study of adults with unresolved/disorganized attachment found altered resting-state connectivity: lower connectivity between the left amygdala and cerebellum, and higher connectivity between the right amygdala and anterior cingulate cortex—patterns present even without clinical psychopathology.
Disorganized attachment also produces a flattened diurnal cortisol slope (Noce et al., 2023), meaning the stress response system stays chronically dysregulated rather than following healthy peaks and valleys. At the autonomic level, Porges' polyvagal theory describes what happens: sympathetic activation (fight/flight) and dorsal vagal shutdown (freeze/collapse) fire simultaneously—the "fear without solution" state that produces the narrowest window of tolerance of any attachment style.
Sensorimotor Psychotherapy (Ogden and Fisher, 2015) and Somatic Experiencing (Levine) work by completing the defensive action sequences that froze in childhood—the reach toward the caregiver that stopped mid-motion, the recoil that never fully discharged. To understand more about how your attachment style affects your nervous system, see our dedicated article.
Pendulation Practice (somatic/body-based, for disorganized attachment)
- Sit comfortably and notice an area of tension or bracing in your body—this often represents the "avoid" impulse. Common locations: jaw, shoulders, chest, belly
- Now find an area that feels neutral or relatively okay—maybe your hands, your feet on the floor, or the backs of your knees
- Slowly shift your attention between the two: 20 seconds on the tension, 20 seconds on the neutral area
- Notice if the tension changes quality—it might soften, shift location, or intensify briefly before releasing
- If you feel a sudden urge to move—push away, curl up, reach out—let the movement happen slowly and deliberately
Pendulation is a core Somatic Experiencing technique that builds the autonomic flexibility disorganized attachment disrupts. By deliberately moving between activation and rest, your nervous system practices the state-shifting that was impossible when both approach and avoidance fired simultaneously. Even 30 seconds of this practice teaches your body that it can move through activation rather than getting stuck in it.
How Does IFS Address the Inner Fragmentation of Disorganized Attachment?
IFS addresses disorganized attachment by working directly with the protector parts and exile parts that embody the contradictory impulses—without forcing premature integration.
When you push people away while wanting them close, that is not one confused feeling. In IFS terms, it is two distinct parts with opposing agendas. A firefighter part may create distance through anger, withdrawal, or numbness to prevent the vulnerability that once led to harm. Meanwhile, an exile part holds the unbearable longing for connection and the grief of never having received safe love.
The "Inner Loving Parent" concept, examined in a study on disorganized attachment and closeness terror, offers a framework for what IFS calls Self-energy—the calm, curious, compassionate presence that can hold space for both parts without being hijacked by either. In IFS, this Self corresponds to the ventral vagal social engagement state described by polyvagal theory.
What makes IFS uniquely suited for disorganized attachment is its respect for the survival function of every part. A protector that shuts down intimacy developed for a reason—your system needed it. The fawn response, for instance, functions as a protector part that appeases to prevent danger. IFS does not try to eliminate these parts. It helps them update their strategies once they trust that Self-energy can lead.
Parts Dialogue (for disorganized attachment)
- When you notice the push-pull—wanting someone close but feeling the urge to flee—pause
- Speak internally to the part that wants connection: "I see you. What do you need right now?"
- Wait. Notice what comes—an image, a sensation, words, or just a feeling
- Now speak to the part that wants to flee: "I see you too. What are you protecting me from?"
- Again, wait and notice
- See if a third quality emerges—something calmer, more curious than either part. That is Self-energy
- From that place, acknowledge both parts: "You both matter. You both kept me alive."
Internal witnessing capacity—the ability to observe contradictory parts without being hijacked by them—is what this exercise builds. For disorganized attachment, the goal is not to resolve the contradiction—it is to create enough internal space that the contradiction no longer controls you. You do not rewire this pattern in a single insight. You rewire it by noticing 10 percent earlier, responding 10 percent differently, 10 percent more often.
When Should You Choose Individual Therapy vs. Couples Therapy?
Individual trauma work typically needs to come before or alongside couples therapy for disorganized attachment. Unlike the anxious-avoidant trap, where couples therapy can address the dynamic directly, disorganized partners often need to stabilize their own nervous system before the relational work can hold.
Johnson, the developer of Emotionally Focused Therapy, notes that disorganized partners "fear both abandonment and danger"—creating a fear-based pursue-withdraw cycle distinct from the standard anxious-avoidant dynamic. One moment they desperately pursue reassurance; the next, they shut down or lash out because the very closeness they sought triggers terror. EFT addresses this, but a partner who dissociates during conflict or cannot stay regulated for a 10-minute conversation may not yet be able to engage in the EFT process.
Jorgensen's adaptation of EFT to attachment styles suggests that disorganized partners benefit most when their individual therapist and couples therapist communicate. The couples work provides a real-time laboratory for practicing new relational patterns, while individual work processes the trauma that drives the old ones.
EFT's outcomes are strong: 77 percent of couples achieve full recovery and 90 percent show significant improvement (Johnson). For a deeper dive into couples-focused approaches, see our article on therapy for anxious-avoidant couples.
Relationship Readiness Assessment (for disorganized attachment)
- Can you identify when you are triggered in your relationship—or do you find yourself suddenly "gone," dissociated, or in a rage without warning? If the latter, start with individual therapy
- Can you stay present during a 10-minute conflict conversation without shutting down completely or escalating? If not, individual stabilization comes first
- Does your partner understand attachment styles and show willingness to learn? If yes, parallel individual plus couples work may be effective
- Have you completed Phase 1 stabilization with an individual therapist—meaning you can identify emotions, tolerate moderate distress, and trust at least one person? If yes, couples therapy can be highly productive at this stage
Disorganized attachment makes this readiness question uniquely high-stakes. Starting couples work too early can replicate the original wound—being in an intimate dynamic without the internal resources to stay safe. There is no shame in saying "I need individual work first." That recognition is itself a sign of growing security.
How Do You Find the Right Therapist for Disorganized Attachment?
The right therapist for disorganized attachment provides a corrective attachment experience—consistent, predictable, non-frightening presence that your nervous system can gradually learn to trust. What matters most is not the modality but the therapist's capacity to be that safe base.
Look for therapists trained in at least one trauma-informed modality—EMDR, IFS, Somatic Experiencing, or Sensorimotor Psychotherapy—who explicitly understand attachment theory. Generic "I work with relationships" is not enough. Ask whether they use a phase-based treatment model and whether they are trained in dissociation, since disorganized attachment frequently involves dissociative responses that untrained therapists can misread as resistance.
Red flags include therapists who push for trauma processing in the first few sessions, who interpret your boundary-setting as avoidance, or who offer a rigid 12-session model for relational trauma that took decades to develop.
The first 3 sessions are a trial. Notice whether you feel slightly safer each time—even if uncomfortable—rather than whether you "like" the therapist. Your disorganized pattern will likely produce an urge to flee after the first or second session. That urge is information, not a verdict. Rupture-repair cycles—moments where the therapeutic relationship hits a snag and you work through it together—are where the deepest healing happens.
Therapist Interview Checklist (for disorganized attachment)
- Start with the broadest question: "What is your approach to working with attachment trauma?" Listen for specificity—attachment theory knowledge, not just "trauma-informed"
- Ask: "How do you handle it when a client dissociates or shuts down in session?" Look for calm, non-pathologizing responses that describe grounding techniques
- Ask: "Do you use a phase-based treatment model?" This reveals whether they understand that stabilization must precede processing
- Ask: "What modalities are you trained in?" Look for EMDR, IFS, Somatic Experiencing, Sensorimotor Psychotherapy, or EFT
- Pay attention to their comfort level when you ask: "How long do you typically work with clients who have relational trauma?" Openness to long-term work matters more than a specific number
These questions specifically screen for the competencies disorganized attachment requires. A therapist's response to question two is particularly revealing—if they seem uncomfortable with dissociation or frame it as "not engaging," they may not have the training your pattern needs.
| Therapy | Evidence Tier | Evidence Type | Best For | Treatment Phase | Format | Typical Duration |
|---|---|---|---|---|---|---|
| EMDR/AF-EMDR | Tier 1 | AAI-measured change | Trauma reprocessing | Phase 2 | Individual | 10–15 sessions (within longer treatment) |
| EFT | Tier 1 | RCT (couples) | Couples work | Phase 3 | Couples | 10–20 sessions |
| IFS | Tier 2 | Clinical rationale | Inner fragmentation | Phase 2 | Individual | Ongoing |
| Sensorimotor Psychotherapy | Tier 2 | Clinical rationale | Body-stored patterns | Phase 2 | Individual | Ongoing |
| Somatic Experiencing | Tier 2 | Clinical rationale | Autonomic dysregulation | Phase 1–2 | Individual | Ongoing |
| Schema Therapy | Tier 2 | Clinical rationale | Core belief schemas | Phase 2 | Individual | 1–3 years |
| DBT | Tier 3 | Adjunct | Distress tolerance skills | Phase 1 | Individual or group | 6–12 month skills module |
When Should You Seek Professional Help for Disorganized Attachment?
Seeking help when you fear attachment figures is paradoxical—and that paradox is itself the signature of disorganized attachment. Your nervous system learned that the people you depend on are dangerous. Asking for help from a new person activates the same ancient alarm. That response makes complete sense given what you experienced.
And recognizing the paradox is the first step through it.
Consider professional support if your relationships consistently end in the same painful pattern—intense connection followed by sudden withdrawal or explosive conflict. Dissociation during conflict, chronic difficulty identifying your own emotions, or a persistent sense of emptiness alongside desperate longing all point toward a disorganized pattern that self-help alone may not resolve.
Co-occurring conditions matter for therapy selection. Disorganized attachment has significant overlap with borderline personality features, complex PTSD, and dissociative experiences. Approximately 76 percent of individuals in clinical treatment carry an unresolved/disorganized AAI classification (AAI meta-analysis), and 42 percent of adults with disorganized attachment report often or always lacking companionship (YouGov survey). You are not alone in this, even when the pattern makes you feel utterly alone.
The pattern predicts therapy dropout. If you have started and stopped therapy multiple times, that is not personal failure—it is the disorganized pattern doing exactly what it was designed to do: pulling you away from attachment figures before they can hurt you. Naming this pattern with your next therapist, in the very first session, changes the dynamic. It turns the obstacle into the material.
Frequently Asked Questions
Can disorganized attachment be healed?
Yes. Research shows adults can shift from disorganized to earned secure attachment through sustained therapeutic work. Wesselmann and Potter (2009) documented AAI-measured change after 10–15 EMDR sessions over approximately one year. Healing requires addressing both the trauma origins and the contradictory relational patterns that sustain insecurity.
Is disorganized attachment the same as fearful-avoidant?
They overlap significantly but come from different research traditions. "Disorganized" (Main and Hesse) comes from infant observation and the Adult Attachment Interview. "Fearful-avoidant" (Bartholomew and Horowitz, 1991) comes from adult self-report measures. Both describe high anxiety and high avoidance, with the same core experience of wanting closeness while fearing it.
How long does it take to heal disorganized attachment?
Most clinicians estimate 1–2 or more years of consistent therapy. Disorganized attachment requires a phase-based approach where stabilization alone can take 3–6 months before trauma processing begins. The timeline depends on trauma severity, co-occurring conditions, and the quality of the therapeutic relationship.
Is EMDR good for attachment issues?
EMDR is the only modality with published evidence of AAI-measured attachment status change in adults with disorganized attachment (Wesselmann and Potter, 2009). Attachment-Focused EMDR (Parnell, 2008) specifically targets relational trauma by building internal attachment resources before processing. It also helps by reprocessing the specific memories that created insecure patterns.
Does IFS help with attachment trauma?
IFS is well-suited for disorganized attachment because its "parts" framework maps directly onto the contradictory impulses—protector parts that push people away coexisting with exile parts that desperately want connection. Research on the "Inner Loving Parent" concept shows it can moderate the closeness terror characteristic of disorganized attachment.
Why is disorganized attachment so hard to heal?
Disorganized attachment creates a neurobiological paradox where the attachment system simultaneously activates approach and avoidance. Brain imaging shows enlarged amygdala volume and altered prefrontal-amygdala connectivity (Noce et al., 2023). The therapeutic relationship itself triggers the wound—since therapists become attachment figures—making consistent engagement uniquely difficult.
Can somatic therapy help with disorganized attachment?
Body-based therapies like Sensorimotor Psychotherapy (Ogden and Fisher, 2015) and Somatic Experiencing are particularly effective because disorganized attachment patterns are stored as incomplete defensive responses in the body. Neuroscience research shows flattened cortisol slopes and simultaneous sympathetic and dorsal vagal activation that talk therapy alone cannot address.
What type of therapist is best for attachment issues?
Look for therapists trained in trauma-informed modalities—EMDR, IFS, Somatic Experiencing, or Sensorimotor Psychotherapy—who explicitly understand attachment theory. For disorganized attachment specifically, the therapist should use a phase-based approach, be comfortable with slow pacing and rupture-repair cycles, and have training in recognizing and working with dissociation.
Want to Go Deeper?
Meadow includes a structured assessment to help you understand your specific attachment patterns, followed by a 66-day program of daily practices designed to build earned security.
Start your free week →References
Attachment Theory and Classification
-
Main, M., & Hesse, E. (1990). Parents' unresolved traumatic experiences are related to infant disorganized attachment status: Is frightened and/or frightening parental behavior the linking mechanism? In M. T. Greenberg, D. Cicchetti, & E. M. Cummings (Eds.), Attachment in the preschool years: Theory, research, and intervention (pp. 161–182). University of Chicago Press.
-
Bartholomew, K., & Horowitz, L. M. (1991). Attachment styles among young adults: A test of a four-category model. Journal of Personality and Social Psychology, 61(2), 226–244.
-
Bakermans-Kranenburg, M. J., & van IJzendoorn, M. H. (2009). The first 10,000 Adult Attachment Interviews: Distributions of adult attachment representations in clinical and non-clinical groups. Attachment & Human Development, 11(3), 223–263.
-
van IJzendoorn, M. H., Schuengel, C., & Bakermans-Kranenburg, M. J. (1999). Disorganized attachment in early childhood: Meta-analysis of precursors, concomitants, and sequelae. Development and Psychopathology, 11(2), 225–249.
EMDR Evidence
-
Wesselmann, D., & Potter, A. E. (2009). Change in adult attachment status following treatment with EMDR: Three case studies. Journal of EMDR Practice and Research, 3(3), 178–186.
-
Scelles, C., & Bherer, L. (2022). EMDR and attachment security: A pilot study. Journal of EMDR Practice and Research, 16(4), 196–210.
-
Parnell, L. (2008). Tapping in: A step-by-step guide to activating your healing resources through bilateral stimulation. Sounds True.
EFT Evidence
-
Johnson, S. M. (2019). Attachment theory in practice: Emotionally focused therapy (EFT) with individuals, couples, and families. Guilford Press.
-
Jorgensen, R. (n.d.). Made to measure: Attachment styles in couples therapy. Retrieved from drrebeccajorgensen.com.
Neuroscience
-
Noce, A. S., et al. (2023). The neurobiology of disorganized attachment: A review. Frontiers in Psychology, 14, 1–15. PMC9947683.
-
Resting-state fMRI study on unresolved/disorganized attachment and amygdala connectivity. (2021). Attachment & Human Development. PMC8615787.
-
Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. W. W. Norton.
Body-Based Therapies
-
Ogden, P., & Fisher, J. (2015). Sensorimotor psychotherapy: Interventions for trauma and attachment. W. W. Norton.
-
Levine, P. A. (2010). In an unspoken voice: How the body releases trauma and restores goodness. North Atlantic Books.
-
Herman, J. L. (1992). Trauma and recovery: The aftermath of violence—from domestic abuse to political terror. Basic Books.
IFS
-
Schwartz, R. C. (1995). Internal family systems therapy. Guilford Press.
-
Disorganized attachment style and the moderating effect of the Inner Loving Parent on closeness terror: An Internal Family Systems (IFS) approach. (2023). Academia.edu.
Epidemiology and Comorbidity
-
YouGov. (2023). What do Americans say about their attachment style? YouGov Survey.
-
Bakermans-Kranenburg, M. J., & van IJzendoorn, M. H. (2017). Preventive interventions for disorganized attachment. In H. Steele & M. Steele (Eds.), Handbook of attachment-based interventions. Guilford Press.
This article is for educational purposes only and does not constitute medical or psychological advice. Disorganized attachment often co-occurs with complex trauma, dissociative experiences, and other conditions that require professional assessment. If you are experiencing dissociation, self-harm, or suicidal thoughts, please contact a licensed mental health professional or crisis service immediately.
