
Internal Family Systems therapy is a psychotherapy model that helps with attachment trauma by treating the mind as a system of protective "parts" organized around a core Self — an inner source of calm, compassion, and clarity. In a pilot study of 17 adults with childhood trauma, Hodgdon et al. (2022) found that 92 percent no longer met PTSD criteria after 16 weekly IFS sessions, with significant reductions in depression, dissociation, and affect dysregulation.
If you have tried talk therapy and understand your attachment patterns intellectually but cannot shift them in your body or your relationships, IFS offers a different entry point. Rather than narrating your story from the outside, IFS works directly with the parts carrying implicit, body-held attachment memories — the ones that drive your protective patterns before your conscious mind catches up. The growing research base, while still limited, suggests this approach may be uniquely suited to the kind of relational wounds that shape how you connect with others.
Key takeaway: Early research suggests IFS can help with attachment trauma by building an internal secure base — your Self provides the attunement caregivers did not. A pilot study found 92 percent of participants no longer met PTSD criteria after 16 sessions, though evidence remains limited. IFS maps naturally onto attachment patterns, with specific parts corresponding to anxious hyperactivation and avoidant deactivation.
What Is IFS and How Does It Relate to Attachment?
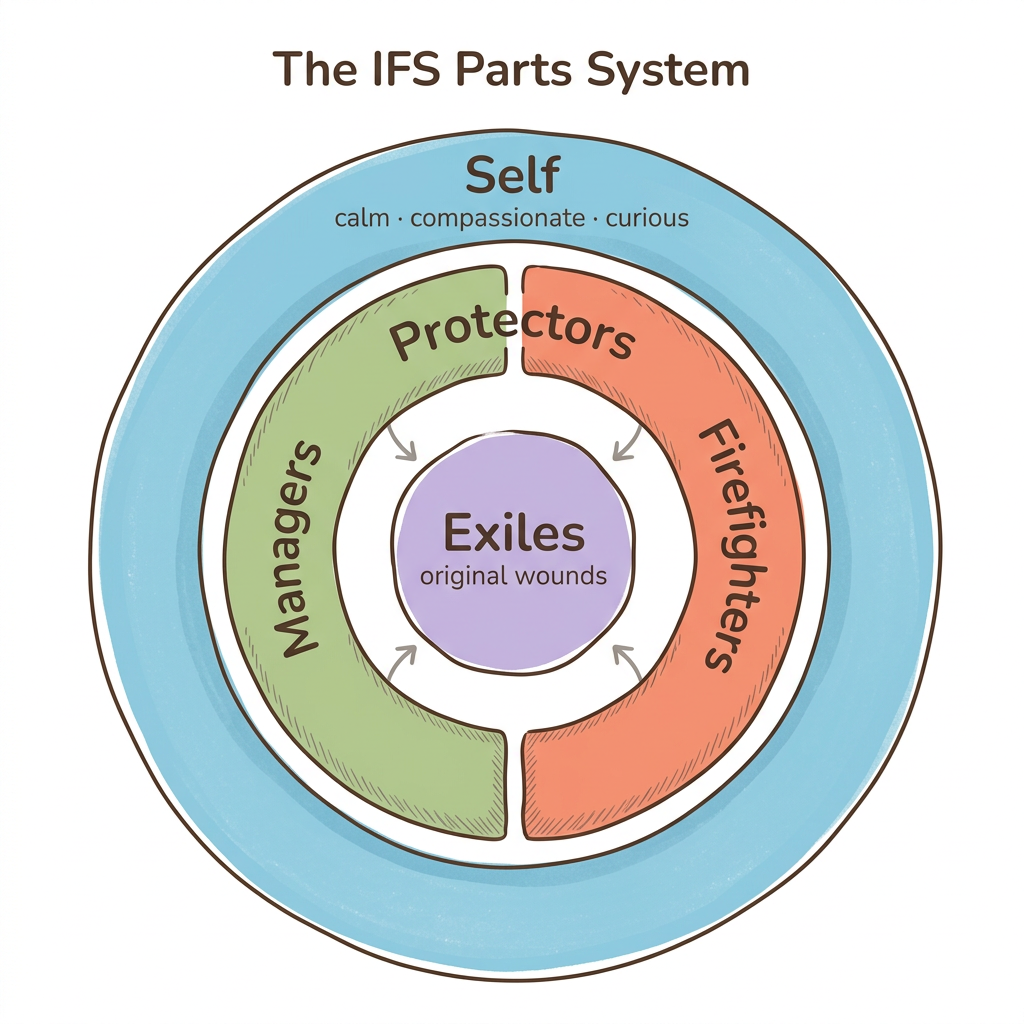
IFS views your mind as naturally containing multiple "parts" — sub-personalities that carry different emotions, beliefs, and roles — organized around a core Self that is inherently whole, wise, and compassionate. Richard Schwartz, who developed the model, identified 8 C's of Self-energy: calm, curious, clear, compassionate, confident, creative, courageous, and connected. These qualities mirror what attachment researchers call a "secure base" — the steady, attuned presence that healthy caregivers provide.
This parallel is not a coincidence. The internal secure base that IFS builds through Self-energy functions the same way an attuned caregiver does: it witnesses pain without being overwhelmed by it, stays present during distress, and offers safety without conditions. For those who did not receive consistent attunement in childhood, IFS offers something radical — the possibility of providing that attunement to yourself, from the inside out.
The model organizes parts into three categories. Protectors include managers (parts that plan, control, and prevent vulnerability) and firefighters (parts that react urgently when pain breaks through — through numbing, distraction, or impulsive behavior). Exiles are younger parts carrying the original wounds — the abandonment, rejection, or terror from early attachment experiences. Protectors work relentlessly to keep exiles locked away, because the pain they hold feels unbearable.
What makes IFS particularly relevant for attachment work is that your protectors likely developed their strategies in response to your earliest relationships. The way you pursue or withdraw in adult relationships is not a personality flaw. Your parts learned those patterns to survive. IFS helps you develop a secure internal relationship with those parts — which, over time, can shift how you relate to others.
Meet Your Self-Energy (for all attachment styles)
Sit comfortably and take three slow breaths. Review the 8 C's — calm, curious, clear, compassionate, confident, creative, courageous, connected — and notice which quality feels most accessible right now, even slightly. Then notice which feels most distant. Without trying to change anything, simply acknowledge: "Right now I have more access to [quality] and less access to [quality]."
This is not parts work yet — it is calibrating your access to Self-energy. For anxious attachment, "calm" and "confident" often feel distant. For avoidant attachment, "connected" and "compassionate" may feel harder to reach. Whatever you notice is information, not a problem to fix.
How Does IFS Map Onto Different Attachment Styles?
Each attachment style corresponds to a distinct configuration of protectors and exiles within the IFS framework — and understanding your particular configuration can transform how you relate to your own patterns. Rather than seeing your attachment style as a fixed label, IFS reveals it as an organized system of parts doing their best to manage old wounds.
Here is how IFS maps onto each attachment style:
-
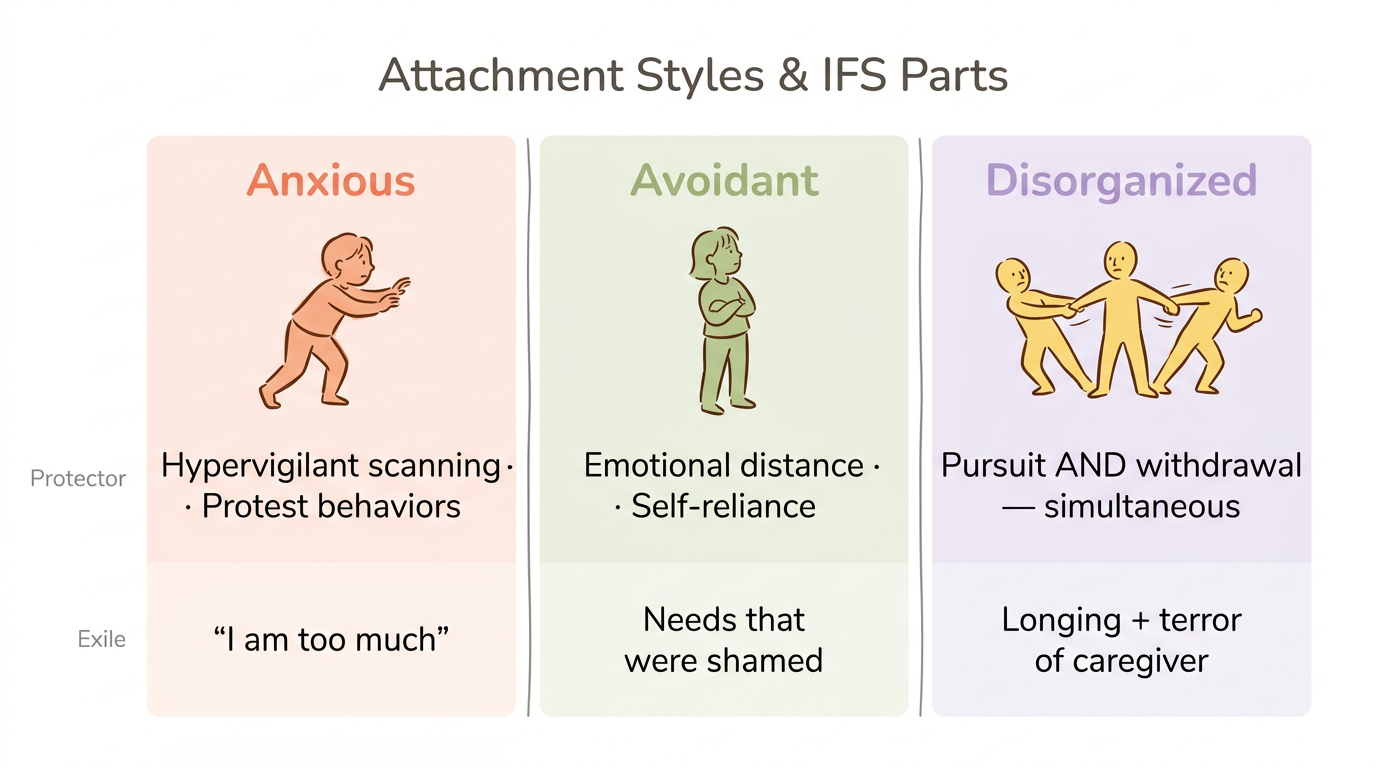
Anxious attachment — hyperactive protector parts. The wound at the center is abandonment — young exiles carrying the belief "I am too much" or "if I stop reaching, I will be forgotten." To keep that pain buried, manager parts scan constantly for signs of rejection, abandonment, or disinterest, driving reassurance-seeking and hypervigilance about your partner's mood. When a threat is detected, firefighter parts flood you with panic or push you toward protest behaviors. When your partner takes two hours to respond to a text, a panicking protector part hijacks your nervous system before you can think clearly.
-
Avoidant attachment — deactivating manager parts. What triggers the whole system is intimacy getting too close. A partner says "I need you" and instantly, manager parts create emotional distance, intellectualize the moment, and default to self-reliance — strategies they learned when showing needs led to rejection or engulfment. If those managers cannot hold the line, firefighter parts numb out through work, substances, or withdrawal. Buried beneath all of it are exiles carrying needs that were shamed — parts that still want closeness but learned it was dangerous to ask. What looks like pushing people away is actually a protector doing its job with fierce dedication.
-
Disorganized attachment — conflicting protector-exile systems. This is where IFS becomes especially clarifying, because the system itself is at war. Parts that desperately want connection AND parts that are terrified by it activate simultaneously, creating the push-pull that defines this style. Manager parts might alternate between pursuit and withdrawal within the same conversation. Exiles carry both the longing for the caregiver and the terror of the caregiver, because the source of comfort was also the source of threat. This is why disorganized attachment feels so confusing — it is not one pattern but multiple parts in conflict.
Parts Mapping by Attachment Style (for all attachment styles)
- Recall a recent moment when you felt triggered in a relationship — a text left on read, a partner pulling away, a moment of unexpected closeness
- Notice the first protective response that arose. Did you pursue? Withdraw? Freeze? People-please?
- Place your hand where you feel that response in your body
- Internally ask that protector part: "What are you afraid would happen if you didn't do your job right now?"
- Notice the vulnerability underneath — the younger feeling the protector is guarding
For anxious attachment, you might hear: "If I stop reaching out, they'll leave and I'll be alone." For avoidant attachment, you might hear: "If I let them in, I'll lose myself" or "They'll see I'm not enough." For disorganized attachment, you may hear contradictory answers — and that is the most important information of all.
What Does the Research Actually Say About IFS for Trauma?
The evidence for IFS in treating attachment-related trauma is promising but limited — and being honest about that distinction matters more than overselling results. The research base is growing faster than most people realize, but it has not yet reached the level of established trauma therapies like EMDR or prolonged exposure.
The most cited study is Hodgdon et al. (2022), a pilot study of 17 adults with PTSD stemming from multiple childhood traumas. After 16 weekly 90-minute IFS sessions, 92 percent no longer met PTSD criteria at one-month follow-up. The effect sizes were striking — d = −4.46 for clinician-assessed PTSD, d = −1.51 for depression, and d = 0.72 for self-compassion. However, this was an uncontrolled study with a small sample, meaning the effect size of d = −4.46 should be interpreted cautiously. There was no comparison group, and some improvement may reflect natural recovery or placebo effects.
Stronger evidence comes from the PARTS Program RCT. Comeau et al. (2024) randomized 60 participants to online group-based IFS or an active control and found significant PTSD symptom reductions comparable to CBT and EMDR, with higher attendance and satisfaction than the control group. Ally et al. (2025) added another piece, showing that online group IFS for comorbid PTSD and substance use produced significant reductions in PTSD severity, linked specifically to increases in emotion regulation, self-compassion, and decentering.
A 2025 scoping review published in the Australian and New Zealand Journal of Family Therapy identified 27 peer-reviewed IFS studies — 17 case studies, 5 quasi-experimental, 3 qualitative, and 2 RCTs. The review concluded that IFS shows promise for PTSD, depression, chronic pain, and self-compassion, but called for larger, more rigorous trials.
The honest assessment: IFS works through mechanisms that align well with what we know about changing attachment styles — building self-compassion, improving emotion regulation, and reprocessing traumatic memories. The early results are encouraging. Larger trials are needed before IFS can claim the same evidence base as more established approaches.
Evidence-Informed Expectations (reflective exercise for all attachment styles)
What I hope IFS will do Supported by current evidence? Might need complementary approaches? Write your hope here Reduced PTSD symptoms, increased self-compassion, improved emotion regulation, greater interoceptive awareness — these are supported Couples work for relational patterns, somatic therapy for deeply body-held trauma — these may need additional modalities Fill in the left column with your personal hopes. Check each one against the middle and right columns. Then sit with the tension of holding both genuine hope and realistic expectations at the same time.
If you noticed yourself hoping IFS would be the answer, that makes sense — anxious parts look for certainty. Your healing does not depend on any single method being perfect. It depends on showing up consistently with good-enough tools.
How Does IFS Work With the Nervous System?
Self-energy access shifts your nervous system from survival states into what polyvagal theory calls the ventral vagal state — the regulated, socially engaged state where connection feels safe rather than threatening. When you access Self, your prefrontal cortex comes online to regulate limbic (amygdala) activation, reducing the hyperarousal that drives anxious protest and the shutdown that drives avoidant withdrawal.
Your protector parts correspond to specific nervous system states. Manager and firefighter parts that pursue, scan for danger, or react with urgency operate from sympathetic activation — the fight-or-flight branch. Parts that numb, dissociate, or collapse into helplessness operate from dorsal vagal activation — the freeze-or-shutdown branch. Self-energy is not another survival state. It is the regulated ground from which you can witness these activations without being hijacked by them. Understanding how your attachment style affects your nervous system makes this mapping even clearer.
One of the most significant findings from the Hodgdon et al. (2022) study was improved interoceptive awareness — the ability to accurately read your body's signals — with effect sizes ranging from d = 0.27 to d = 1.21. This matters because attachment trauma disrupts body-signal reading. If your caregiver's emotions were unpredictable or overwhelming, your nervous system may have learned to dampen or distort body signals as protection. IFS helps reverse this by bringing curious, compassionate attention back to what your body is communicating.
Research on self-compassion physiology — which parallels the Self-energy state — shows decreased cortisol and increased oxytocin release when you engage a compassionate orientation toward your own suffering. Frank Anderson's work on IFS neurobiology suggests that what IFS calls "parts" may map onto distinct neural subsystems revealed by qEEG and fMRI research — some evolutionarily ancient, some shaped by childhood attachment experiences. IFS facilitates memory reconsolidation — the process by which traumatic implicit memories are accessed and reprocessed with Self-energy, promoting adaptive neural rewiring.
Your window of tolerance expands as Self-energy becomes more accessible. Not because the painful memories disappear, but because your system develops a larger container for holding them.
Somatic Parts Check-In (body-based technique for all styles, especially avoidant and disorganized)
Place one hand on your chest and notice your breathing rate — fast, slow, shallow, deep — without changing it. Slowly scan from your head down to your feet, noticing areas of tension, numbness, buzzing, heaviness, or warmth. When you find a sensation that stands out, pause there and silently ask: "Which part is holding this?" Breathe toward that area with curiosity rather than trying to fix or release it — just "I see you." Notice whether the sensation shifts, stays, or intensifies when you bring compassionate attention to it.
This engages interoceptive awareness — the body-signal reading that attachment trauma disrupts. For avoidant attachment, this reconnects you with body signals your system learned to mute. For disorganized attachment, it builds the interoceptive capacity that helps you distinguish between "I am in danger" and "my body is remembering danger." Even 30 seconds of this practice builds the neural pathways of Self-to-body attunement.
How Is IFS Different from Other Trauma Therapies?
IFS is the only major trauma therapy that specifically builds an internal relationship system — treating healing as a process of relating to your own parts with the attunement and compassion that early caregivers did not provide. Other approaches access and process trauma through different mechanisms, and understanding these differences helps you choose what fits your needs.
| Feature | IFS | EMDR | Somatic Experiencing | EFT (Couples) |
|---|---|---|---|---|
| Primary focus | Internal parts system and Self-leadership | Specific traumatic memories | Nervous system discharge and regulation | Couple attachment bonds |
| Best for attachment style | All styles, especially disorganized | Specific attachment injuries | Avoidant (body reconnection) | Anxious-avoidant dynamics |
| How it accesses trauma | Through parts carrying implicit memory | Bilateral stimulation and memory reprocessing | Body sensation tracking | Emotional engagement in session |
| Evidence base | Promising — 2 RCTs, multiple pilots | Strong — 30 or more RCTs | Moderate — growing | Strong for couples — 20 or more RCTs |
| Self-guided potential | Moderate (protector work only) | Low (requires clinician) | Low to moderate | Low (requires both partners and therapist) |
| Typical duration | 16 to 30 or more sessions | 8 to 16 sessions | 12 to 24 sessions | 12 to 20 sessions |
| Unique strength | Builds internal secure base | Rapid single-event processing | Completes incomplete survival responses | Repairs current relationship bonds |
IFS and EMDR integration is becoming increasingly common for complex attachment trauma. IFS addresses the fragmented internal system — the parts that carry conflicting attachment needs — while EMDR processes the specific memories those parts hold. Many clinicians find this combination more effective than either approach alone, particularly for disorganized attachment where both the internal conflict and the traumatic memories need attention.
What does this look like in practice? For couples caught in the anxious-avoidant trap, individual IFS work can complement couples therapy approaches like EFT. IFS helps each partner understand and soften their own protective parts, while EFT creates the relational safety for new attachment experiences together.
These approaches are not mutually exclusive. An integrative approach — IFS for internal parts work, somatic techniques for body-held activation, and EMDR or EFT as needed — often serves attachment trauma better than any single modality. The question is not which therapy is "best" but which combination matches where you are right now.
Therapy Readiness Reflection (self-assessment for all attachment styles)
- Can you notice different "parts" or internal voices when you are activated? If yes, IFS may be a fit
- Do you have specific traumatic memories you can identify and name? EMDR may help process those directly
- Is your distress mostly felt in your body — as tension, numbness, chronic pain, or activation that will not settle? Somatic work may be needed
- Are your attachment patterns showing up primarily in your current relationship? EFT or couples work addresses relational dynamics directly
- Do you experience all of the above? An integrative approach combining modalities may serve you best
This is a starting point for conversation with a therapist, not a prescription. Your answers may also shift depending on what stage of healing you are in — avoidant attachment often benefits from somatic and IFS work early on, adding relational approaches as comfort with vulnerability grows.
Can You Practice IFS on Your Own for Attachment Healing?
Beginner-safe exercises — noticing parts, mapping protectors, and building Self-energy access — can be practiced independently and offer genuine benefit. The line between safe self-practice and work that requires professional support comes down to one distinction: protectors versus exiles.
Your nervous system learned its protective patterns for good reason. Appreciating those parts — rather than trying to override them — is itself a form of healing, and it is something you can do on your own. Jay Earley's Self-Therapy provides structured self-guided exercises for this kind of work, and many people report meaningful shifts just from learning to relate to their protectors with curiosity instead of frustration.
Professional support is required for unburdening — the IFS process of accessing exiled parts, witnessing their pain, and releasing the beliefs and emotions they carry. Exiles hold your deepest attachment wounds, and approaching them without a trained guide can overwhelm your system, retraumatize vulnerable parts, or activate protectors so strongly that the process stalls. Working with parts that carry suicidal ideation, self-harm impulses, or memories of abuse or neglect requires an IFS-trained clinician who can hold the therapeutic container while your system opens.
The protectors versus exiles distinction is your safety guardrail. If you are noticing protectors, appreciating them, and learning what they fear — that is safe self-guided work. If you find yourself flooded with childhood memories, intense grief, or dissociative experiences — that is exile territory, and your system is asking for professional support.
Meadow's tools can complement this process by helping you recognize your attachment patterns and build awareness of which protectors are active in your daily life — without attempting the deeper unburdening work that belongs in a therapeutic relationship.
The Protector Appreciation Practice (daily practice for all attachment styles)
- At some point today, notice when a protector part activates — the urge to check your phone again, to withdraw from a conversation, to say "I'm fine" when you are not, or to over-accommodate someone else's needs
- Internally, name what the part is doing: "There's the checking part" or "There's the distancing part"
- Silently say: "Thank you for trying to protect me. I see you working hard"
For anxious attachment, this might sound like appreciating the reassurance-seeking part: "You're scanning for danger because last time you missed the signs, someone left." For avoidant attachment, it might be the distancing part: "You're creating space because closeness used to mean losing yourself." This practice stays with protectors — it does NOT attempt to access the exiles underneath. That is what makes it safe for self-guided work.
When Should You Seek Professional Help for Attachment Trauma?
You should seek professional support when self-guided parts work begins to access deeper material than your nervous system can hold alone. This is not a failure of effort or insight — it is your system accurately communicating that the work requires a co-regulating presence.
Specific signs that professional help is needed include dissociation during parts work — losing time, feeling detached from your body, or going blank when you try to connect with a part. Overwhelming emotions that do not settle within a reasonable window after self-guided exercises also signal that exiles are surfacing without adequate containment. If your attachment trauma involves abuse or neglect by primary caregivers, the complexity of those wounds generally requires an IFS-certified therapist who can hold the therapeutic relationship as a corrective attachment experience.
Other indicators include using substances or compulsive behaviors to manage what comes up during self-reflection, persistent relationship patterns that repeat despite genuine awareness and effort, or noticing that your window of tolerance narrows rather than expands as you do this work. These are not signs that IFS is wrong for you — they are signs that you need a professional container for the process.
To find an IFS-trained therapist, the IFS Institute maintains a directory organized by certification level. Level 1 practitioners have completed the foundational training; Level 2 and Level 3 practitioners have advanced training in complex trauma. When interviewing potential therapists, ask specifically about their experience with attachment trauma and whether they integrate IFS with other modalities.
The first few sessions typically involve psychoeducation about the IFS model, mapping your primary protectors, and building enough Self-energy access to approach deeper work safely. Therapy can genuinely change attachment patterns — but only when the therapeutic relationship itself becomes a safe base.
Window of Tolerance Check (safety practice — use before and after any self-guided parts work)
- Before beginning, rate your nervous system activation on a scale of 1 to 10 (1 is completely shut down or numb, 10 is completely overwhelmed or panicked)
- If you are above 7 or below 3, pause the parts work — your system is outside its window of tolerance and needs regulation first
- After completing a parts exercise, rate yourself again
- If you have moved further from center (higher or lower than when you started), practice the Somatic Parts Check-In from earlier in this article before continuing your day
- Track your ratings over time — if self-guided work consistently moves you outside your window, that is clear information that professional support would help
This works for all attachment styles but is especially important for disorganized attachment, where the window of tolerance tends to be narrower and fluctuate more rapidly. The rating system builds the interoceptive awareness that helps you become your own safety monitor.
Frequently Asked Questions
Is IFS evidence-based for trauma?
IFS has promising but limited evidence. Hodgdon et al. (2022) found 92 percent PTSD remission after 16 sessions in an uncontrolled pilot. Two RCTs show significant symptom reductions, and a 2025 scoping review identified 27 peer-reviewed studies but called for larger trials.
Can IFS change your attachment style?
IFS can support movement toward earned secure attachment by building an internal secure base through Self-energy. While no studies directly measure attachment style change from IFS specifically, the mechanisms IFS engages — increased self-compassion, improved emotion regulation, reduced trauma symptoms — align with factors research links to attachment security shifts over time.
What's the difference between IFS and EMDR for attachment trauma?
IFS works with the entire internal parts system and builds Self-leadership as an ongoing resource for navigating relationships. EMDR targets specific traumatic memories for reprocessing through bilateral stimulation. For attachment trauma, IFS addresses the relational patterns that parts create, while EMDR processes the specific events that shaped those patterns. Many clinicians working with complex attachment trauma combine both approaches.
Can you do IFS therapy on yourself?
You can safely practice noticing parts, mapping protectors, and building Self-energy access independently. Resources like Jay Earley's Self-Therapy offer structured exercises for this. However, unburdening exiles — the step where deep attachment wounds are processed and released — generally requires professional guidance, especially for complex or childhood trauma. The protectors-versus-exiles distinction is your safety guideline.
Does IFS work for disorganized or fearful-avoidant attachment?
IFS may be particularly well-suited for disorganized attachment because it directly addresses the internal conflict that defines this style — parts that desperately want connection clashing with parts that fear it. Rather than forcing a single narrative, IFS gives each conflicting part a voice and a seat at the table, which mirrors the both-and reality of disorganized attachment experience.
How long does IFS therapy take to work for attachment trauma?
The Hodgdon et al. (2022) pilot study used 16 weekly 90-minute sessions and found significant improvement across PTSD, depression, and self-compassion measures. Most IFS clinicians suggest 6 to 12 months minimum for meaningful shifts in attachment patterns, as these involve deeply rooted protective systems. Complex trauma may require longer treatment. Progress tends to be nonlinear — significant shifts often follow periods that feel stuck.
What are protectors and exiles in IFS?
Protectors are parts that developed strategies to keep you safe. Managers prevent vulnerability through perfectionism, people-pleasing, or emotional distance. Firefighters react urgently when pain breaks through — through numbing, anger, or impulsive behavior. Exiles are younger parts carrying original attachment wounds, holding the abandonment or rejection that protectors work to keep at bay.
How does IFS work with the nervous system?
Self-energy access engages prefrontal cortex regulation over limbic reactivity, shifting you from survival states into the ventral vagal state where connection feels safe. Hodgdon et al. (2022) found IFS improved interoceptive awareness, and self-compassion research shows decreased cortisol and increased oxytocin — supporting the nervous system regulation that attachment healing requires.
Want to Go Deeper?
Meadow includes a structured assessment to help you understand your specific attachment patterns, followed by a 66-day program of daily practices designed to build earned security.
Start your free week →References
Clinical Research
-
Hodgdon, H. B., Anderson, F. G., Southwell, E., Hrubec, W., & Schwartz, R. (2022). Internal family systems (IFS) therapy for posttraumatic stress disorder (PTSD) among survivors of multiple childhood trauma: A pilot effectiveness study. Journal of Aggression, Maltreatment & Trauma, 31(1), 22–43.
-
Comeau, A., et al. (2024). PARTS Program: Online group-based Internal Family Systems for PTSD. Psychological Trauma: Theory, Research, Practice, and Policy.
-
Ally, S., et al. (2025). Online group Internal Family Systems therapy for comorbid PTSD and substance use. Frontiers in Psychiatry.
-
Scoping review (2025). Internal Family Systems therapy evidence base. Australian and New Zealand Journal of Family Therapy.
IFS Theory and Model
-
Schwartz, R. C. The evolution of the Internal Family Systems model. IFS Institute.
-
Earley, J. Self-Therapy: A Step-by-Step Guide to Creating Wholeness and Healing Your Inner Child Using IFS.
Neuroscience and Mechanisms
-
Anderson, F. Internal Family Systems, neuroplasticity, and attachment. Therapist Uncensored Podcast, Episode 182.
-
Porges, S. W. The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation.
-
Calma Again Counseling. The neurobiology of IFS: How it affects trauma recovery.
Attachment-IFS Integration
-
Pasadena Trauma Therapy. Attachment styles and parts work: IFS healing.
-
Life Architect. Attachment trauma and IFS.
-
Sea Change Psychotherapy. Attachment therapy with IFS and EMDR integration.
Clinical Resources
-
IFS Institute. Therapist directory and certification levels.
-
Positive Psychology. Internal Family Systems therapy exercises and worksheets.
This article is for educational purposes only and is not a substitute for professional mental health treatment. If you are experiencing significant distress related to attachment trauma, please consult a licensed therapist trained in IFS or another evidence-based trauma therapy. If you are in crisis, contact the 988 Suicide and Crisis Lifeline by calling or texting 988.
