
Therapy can change your attachment style—and the evidence is stronger than most people realize. In a landmark randomized controlled trial, Levy et al. (2006) found that patients receiving Transference-Focused Psychotherapy shifted from insecure to secure attachment classification after just 12 months, making it the first RCT to demonstrate attachment classification change through therapy. Approximately 50 percent of adults carry insecure attachment patterns (Hazan and Shaver, 1987).
If you've identified your attachment style and you're wondering whether it's permanent, you're asking the right question. Below, you'll find the evidence on which modalities work, how long the process takes, and what changes in your brain and body. For a broader look at attachment change beyond therapy, see Can Your Attachment Style Change Over Time?.
Key takeaway: Therapy can change your attachment style. A randomized controlled trial showed patients shifted from insecure to secure attachment after 12 months of targeted therapy. Approximately 30 percent of adults naturally shift attachment categories over four years, but therapy accelerates this process through corrective relational experiences that update your nervous system and internal working models.
What Does the Research Say About Therapy and Attachment Change?
If you've spent time understanding your attachment style, it's natural to wonder whether the research backs up the possibility of real change. It does. Attachment classification change—shifting from insecure to secure—has been demonstrated in randomized controlled trials, not just clinical anecdotes.
The strongest evidence comes from Levy et al. (2006), who randomized 90 patients with borderline personality disorder into three therapy types: Transference-Focused Psychotherapy, Dialectical Behavior Therapy, and supportive psychotherapy. After 12 months, only TFP patients showed significant increases in secure attachment classification and reflective function. DBT reduced self-harm but did not change attachment patterns. This distinction matters—it suggests that not all therapies are equally effective at reaching the relational core of attachment.
Beyond this landmark trial, the numbers tell a compelling story. Approximately 30 percent of adults shift attachment categories over four years even without targeted intervention (Pinquart et al., 2013). A meta-analysis of 36 studies (N = 3,158) confirmed that improvements in attachment security during therapy coincide with better treatment outcomes across the board (Levy et al., 2018). Fraley's (2002) meta-analysis described a "prototype model" of attachment stability (ρ = 0.39)—meaning early patterns persist as a kind of default setting, but they can be updated with new relational input.
What does earned secure attachment actually look like? About 14 percent of adults in one sample were classified as earned secure—meaning they developed insecure attachment in childhood but achieved secure functioning later in life. Learn more about what earned secure attachment means and what the research shows about its outcomes.
Attachment Timeline Reflection (for all attachment styles—builds reflective functioning)
- Write down three key relationships: your primary childhood caregiver, your first romantic partner, and your current closest relationship
- For each, note your typical response when you felt disconnected—did you pursue, withdraw, or oscillate?
- Notice where patterns repeat and where they've already shifted
- Circle any relationship where your pattern was different from your default
- Ask yourself: what was different about that person or context?
For anxious attachment specifically: notice whether your hypervigilance intensity has varied across these relationships. If it has, your system already knows how to modulate—it's done it before. This reflection builds reflective functioning, the same capacity that TFP targets to produce attachment change (Levy et al., 2006).
How Does the Therapeutic Relationship Itself Change Attachment?
The therapeutic relationship functions as a corrective attachment experience—a live, real-time opportunity for your nervous system to learn that closeness can be safe. The therapist serves as a temporary secure base, offering consistent attunement that most insecurely attached clients did not reliably receive in childhood.
Your attachment patterns are encoded in what researchers call internal working models—implicit templates that predict how others will respond to your needs. When a therapist responds differently than your template expects—staying present when you push away, remaining calm when you escalate, repairing after a misunderstanding—your model begins to update. This process of rupture and repair is not a therapeutic failure. It is the mechanism of change itself.
Levy and Johnson (2018) describe attachment as providing a "comprehensive yet parsimonious foundation for psychotherapy research and practice." Patients with low pretreatment attachment security may find better outcomes in therapies that focus on interpersonal interactions and close relationships—because those therapies directly engage the relational system that needs updating.
Mikulincer and Shaver (2020) demonstrated that even brief activation of secure attachment representations—called security priming—reduces insecure responding and promotes better emotion regulation. Therapy does this repeatedly, session after session, building cumulative change. Over time, the security experienced in the therapeutic relationship generalizes to other relationships. The client doesn't just feel safe with the therapist—they begin feeling safe with others.
Secure Base Visualization (security priming technique—especially valuable for avoidant attachment)
- Close your eyes and bring to mind someone who made you feel genuinely safe and accepted—a therapist, grandparent, friend, teacher, or even a fictional character
- Notice where you feel warmth or softening in your body—chest, belly, hands, face
- Stay with the image for 60 seconds, breathing naturally
- If the image fades, gently return to it without forcing
- Before opening your eyes, notice how your body feels compared to when you started
For avoidant attachment: this exercise may feel uncomfortable, awkward, or "pointless." That discomfort is your deactivating system encountering safety—it's unfamiliar, so your protective pattern dismisses it. The resistance itself is information about your attachment style. Based on Mikulincer and Shaver's (2020) research showing that security priming activates the same neural circuits whether the figure is real or imagined.
Which Therapy Modality Works Best for Each Attachment Style?
The best therapy for attachment issues depends on your specific attachment pattern. Anxious attachment responds to therapies that provide consistent co-regulation and emotional restructuring. Avoidant attachment benefits from approaches that gradually expose vulnerability within a boundaried therapeutic frame. Disorganized attachment requires trauma-informed modalities that address nervous system dysregulation before deepening relational work.
Here is how the major evidence-based modalities compare:
| Therapy Modality | Best For | How It Works | Evidence Level | Typical Duration | Key Strength |
|---|---|---|---|---|---|
| TFP | Avoidant and disorganized | The therapeutic relationship surfaces unconscious relational patterns in real time | RCT (Levy et al., 2006) | 1–2 years | Only therapy proven to change attachment classification in an RCT |
| EFT | Anxious and couples | Emotional responses and bonding cycles are restructured through guided interactions | Meta-analysis (d = 1.3) | 8–20 sessions for couples | Largest effect size of any couples intervention |
| CBT | Anxious (with adjuncts) | Cognitive distortions about relationships are identified and challenged | Multiple RCTs | 12–20 sessions | Widely available, though body-based patterns may need additional modalities |
| Somatic Experiencing | Disorganized and trauma-based | Stored nervous system activation is gradually titrated and released | Growing clinical evidence | Varies | Reaches body-encoded attachment patterns that talk therapy alone cannot access |
| EMDR (Attachment-Focused) | All styles with trauma history | Bilateral stimulation helps reprocess relational trauma memories | Growing RCT data | 8–12 sessions for targeted trauma | Efficient processing of specific relational trauma memories |
| IFS | Disorganized and all styles | Protective parts developed from attachment wounds are explored and "unburdened" | NREPP evidence-based | Varies | Internal system work without requiring immediate relational vulnerability |
The EFT effect size of 1.3 is larger than any other couples intervention studied to date. For couples caught in a pursuit-withdrawal dynamic, EFT directly restructures the attachment bond. If that pattern sounds familiar, read about the anxious-avoidant trap and how couples therapy addresses it.
CBT can reduce attachment insecurity as a byproduct of treating anxiety or depression, but research suggests it may be less effective for avoidantly attached individuals who intellectualize without engaging emotionally. Relationally-oriented adjuncts improve its impact on attachment specifically.
If you identify with disorganized attachment patterns, trauma-informed approaches like somatic experiencing, attachment-focused EMDR, or IFS often need to come before or alongside relational therapies. The nervous system dysregulation in disorganized attachment can be too intense for purely talk-based approaches.
5 Questions to Ask a Potential Therapist About Attachment
- How do you understand attachment theory in your clinical work?
- Do you pay attention to what's happening between us in the room—the therapeutic relationship itself?
- How do you work with ruptures—moments when I feel misunderstood or disconnected from you?
- What's your approach when a client shuts down or becomes emotionally flooded?
- Are you familiar with earned secure attachment, and what does that process look like in your practice?
Therapy Modality Self-Assessment (for all attachment styles)
- Review the comparison table above and identify your primary attachment style
- Read the "Best For" and "How It Works" columns for modalities matching your style
- Note which descriptions resonate with your experience—not just which sound most impressive
- Write down one or two modalities to research further or ask a potential therapist about
- Notice your emotional response to each option—does one feel "too much"? Does one feel "not enough"?
For anxious attachment specifically: notice if you're drawn to the most intensive or longest-duration option. Your protest behavior may seek reassurance that "enough" therapy exists. Any evidence-based modality with a good relational fit between you and your therapist is sufficient. The relationship matters more than the brand name.
What Happens in Your Brain and Body When Attachment Changes?
Attachment change is not just psychological—it is neurobiological. When therapy shifts your attachment patterns, measurable changes occur in your brain's stress response circuits, hormonal systems, and autonomic nervous system regulation.
Oxytocin-mediated circuits play a central role. Early life stress can inhibit oxytocin formation, leading to a hyperactive amygdala with poor prefrontal cortex connectivity—the neural signature of insecure attachment responding. Buchheim et al. found that oxytocin enhances functional connectivity between the amygdala and prefrontal cortex, restoring the brain's capacity to regulate emotional reactions to attachment cues. Therapy helps rebuild these social bonding circuits over time.
Securely attached individuals show cortisol buffering—decreased cortisol release during stress, a neuroendocrine protective effect (Feldman, 2017). Therapy that builds attachment security can restore this buffering, meaning your body literally produces less stress hormone in relational situations that previously felt threatening.
One reason talk therapy alone may be insufficient for deeply ingrained attachment patterns is that attachment is right-hemisphere encoded. Schore's research demonstrates that the right hemisphere grows more rapidly than the left during the first 18 months of life—the primary attachment-formation window. Attachment patterns are stored in implicit, body-based memory systems, not narrative memory. This is why you can understand your patterns intellectually and still find yourself repeating them—the knowledge lives in a different part of your brain than the pattern.
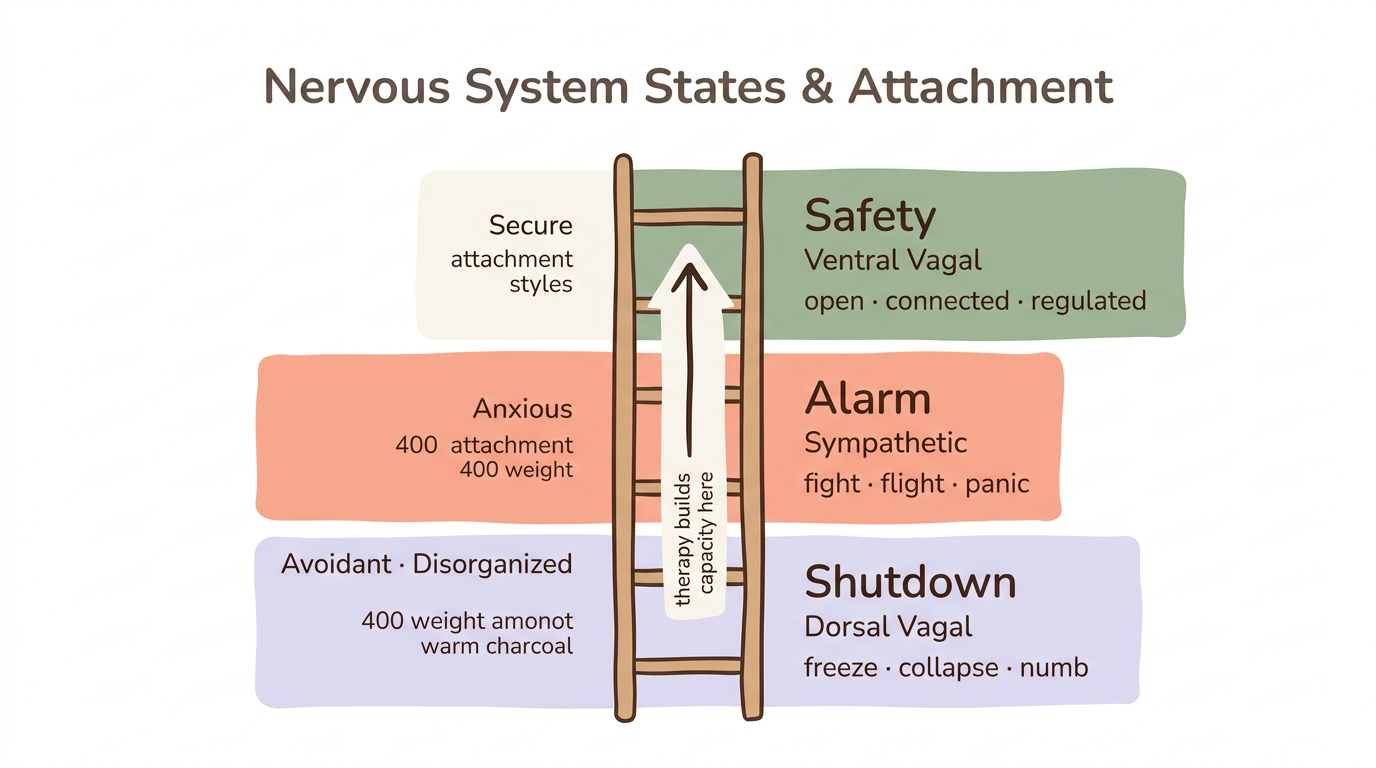
Porges' polyvagal theory offers a framework for understanding attachment at the nervous system level. Insecure attachment often means being stuck in sympathetic activation (fight or flight—common in anxious attachment) or dorsal vagal shutdown (freeze and collapse—common in avoidant and disorganized attachment). Therapy helps clients access the ventral vagal state—the neural platform for feeling safe, socially engaged, and open to connection. The therapist's calm, regulated presence supports co-regulation, gradually teaching your nervous system that it can settle in the presence of another person. For a deeper exploration of these mechanisms, see how attachment style affects your nervous system.
Research on inter-brain synchrony provides another mechanism: therapy improves patients' capacity to achieve neural synchrony with others, and recurring exposure to this synchrony produces lasting change in relational functioning.
Ventral Vagal Activation Practice (somatic technique—especially valuable for disorganized attachment)
- Place one hand on your chest and one on your belly
- Inhale through your nose for 4 counts
- Exhale slowly through your mouth for 6 counts—the longer exhale is what activates the ventral vagal pathway
- On each exhale, let your shoulders drop one millimeter
- After 5 breaths, gently turn your head side to side, letting your eyes take in the room around you—this orienting response signals safety to your nervous system
- Notice any shift in your body: warmth, softening, heaviness, or quiet
This activates the ventral vagal complex—the same neural circuit that therapy helps you access more reliably over time. For disorganized attachment: if you notice oscillation between numbness and agitation during this exercise, your nervous system is toggling between dorsal vagal and sympathetic states. That oscillation is not failure—it is your system's learned protective response. The practice builds capacity to stay in the ventral vagal window for slightly longer each time.
How Long Does It Take for Therapy to Change Attachment?
Your nervous system learned its attachment patterns over years of repeated experience—and updating those patterns requires sustained repetition in the other direction. Clinical consensus places that timeline at one to two years of weekly therapy for meaningful attachment style shift.
The Levy et al. (2006) RCT demonstrated attachment classification change at 12 months—a meaningful benchmark, though that study used intensive psychotherapy with highly trained clinicians. Bakermans-Kranenburg et al. (2003) conducted a meta-analysis of 70 intervention studies (N = 7,636) and found an effect size of d = 0.20 for attachment security and d = 0.33 for parental sensitivity. These are modest but real effects—change happens, and it is measurable, but it is gradual, not sudden.
Earned-secure individuals spent more time in therapy than other attachment categories, according to research on earned security outcomes. This finding aligns with clinical experience: the people who achieve lasting attachment change are the ones who stay in the process long enough for their nervous system to internalize new relational patterns.
Attachment change in therapy tends to unfold in recognizable phases:
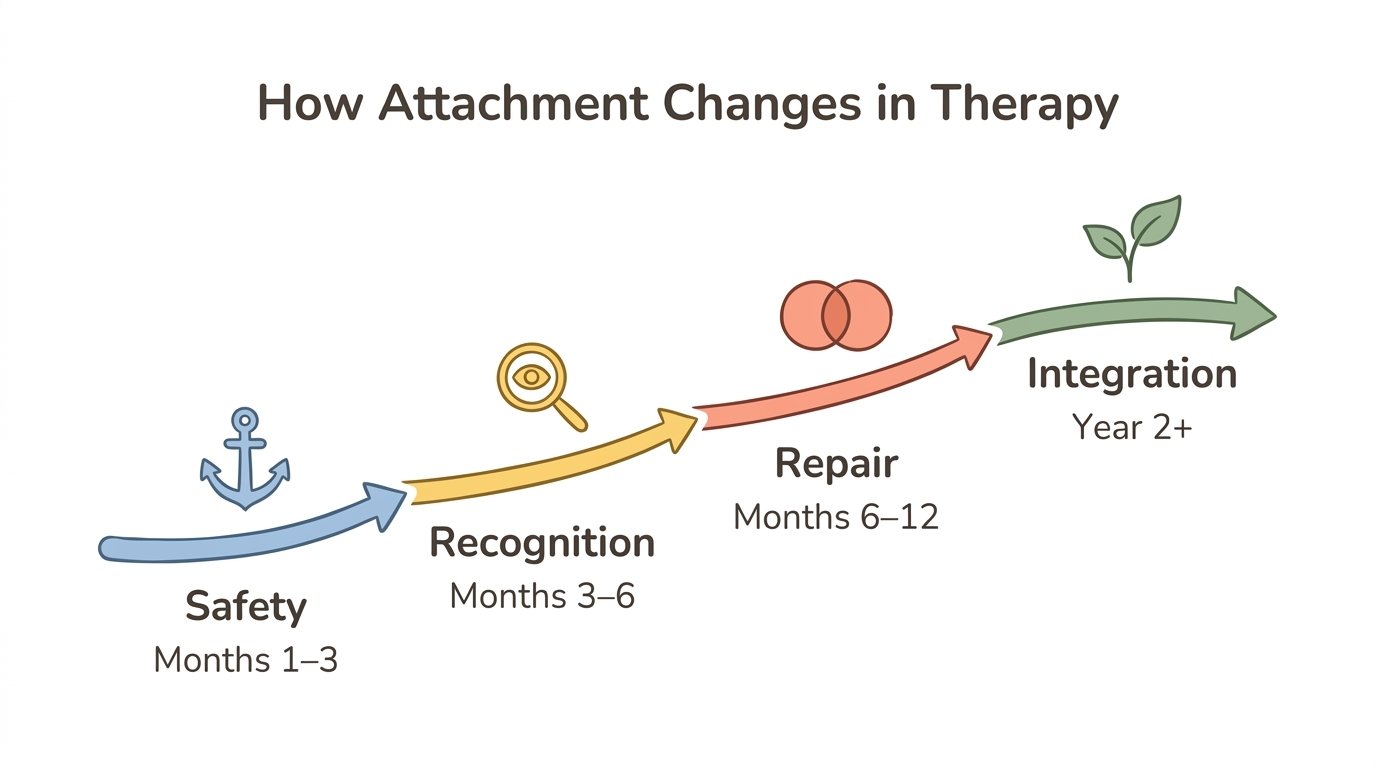
- Alliance building (months 1–3): Establishing safety with the therapist, learning each other's communication styles, beginning to trust the frame
- Pattern recognition (months 3–6): Identifying your attachment responses as they arise in and outside sessions, building reflective functioning
- Corrective experiences and rupture-repair (months 6–12): Experiencing moments of disconnection with the therapist and successfully repairing them—this is where internal working models begin to update
- Integration and generalization (year 2 and beyond): New relational patterns start showing up in relationships outside therapy, becoming more automatic
You don't rewire attachment in a single insight. You rewire it by noticing 10 percent earlier, responding 10 percent differently, 10 percent more often.
Milestone Tracking Journal (for all attachment styles)
- At the start of therapy, write your response to: "When I feel disconnected from someone important, I typically…"
- Write your response to: "My body's first response to emotional closeness is…"
- Date both entries and seal them—do not reread for 3 months
- Every 3 months, write fresh responses to the same prompts without looking at previous answers
- After 6 months, compare your entries side by side and notice what has shifted
For anxious attachment specifically: resist the urge to evaluate progress weekly or after every session. Attachment change operates on a longer timescale than symptom relief, and frequent checking can itself become a reassurance-seeking pattern. Three-month intervals honor the pace at which your nervous system actually integrates new experiences.
Can You Change Your Attachment Style Without Therapy?
Partially, yes—but therapy accelerates and deepens the process. Corrective attachment experiences can occur in any relationship where someone consistently responds to your needs with attunement and reliability. A secure romantic partner, a steady friendship, or even a mentoring relationship can function similarly to therapy by providing a new relational template.
Mikulincer and Shaver's (2020) research on security priming demonstrates that even brief, self-directed exercises—like imagining a secure attachment figure or recalling a moment of genuine safety—reduce insecure responding and improve emotion regulation. This is not wishful thinking. Contextual activation of secure attachment representations produces measurable changes in how people process threat and approach closeness.
Fraley's (2002) prototype model confirms that early attachment patterns persist as defaults but can be updated through new experiences. About 30 percent of adults shift attachment categories over four years without targeted intervention (Pinquart et al., 2013). Change happens—sometimes without professional help.
Mindfulness and somatic practices also regulate the nervous system independently. Between-sessions practice matters enormously: what you do between therapy sessions (or instead of therapy) shapes the pace of change. For between-sessions techniques specific to anxious attachment, see how to self-soothe anxious attachment. For a comprehensive guide to building security through multiple pathways, see how to develop secure attachment as an adult.
However, honesty matters here. Disorganized attachment and patterns rooted in significant relational trauma typically benefit from professional support. The nervous system dysregulation is too intense to navigate alone safely—not because you're incapable, but because your protective system was designed to activate in relationship, and it often needs relationship to heal. Self-help tools like Meadow serve as a complement to therapy, not a replacement—offering structured security priming, nervous system regulation exercises, and pattern tracking between sessions.
Daily Security Priming Practice (Meadow-aligned—especially valuable for avoidant attachment)
- Each morning, spend 2 minutes recalling a moment when you felt genuinely safe with another person
- Notice sensations in your body—warmth, ease, softening, openness
- Let the memory sit for 30 seconds without analyzing it
- Throughout the day, when attachment anxiety or avoidance activates, briefly return to this memory for 10–15 seconds
- At the end of the day, note what triggered the activation and how quickly you returned to baseline
For avoidant attachment: if no memory comes easily, use an imagined ideal—a person who would respond to you exactly as you needed. Mikulincer and Shaver's (2020) research shows imagined secure figures activate the same neural circuits as real ones. The difficulty in accessing these memories is itself a feature of your deactivating system, not evidence that safety never existed.
When Should You Seek Professional Help for Attachment Patterns?
Your attachment patterns developed for good reason—they kept you safe in environments where safety wasn't guaranteed. And if those patterns are now causing significant distress, professional support can offer something that self-work alone often cannot: a live relationship in which to practice being different.
Consider seeking an attachment-informed therapist if any of the following resonate:
- Repeated breakups, chronic conflict, or isolation stemming from attachment patterns that cause significant relationship distress
- Attachment reactions that feel physically overwhelming—panic, dissociation, rage, or emotional numbness beyond your capacity to regulate
- A history of relational trauma or abuse in childhood caregiving relationships
- Disorganized attachment patterns—simultaneous urges to seek closeness and flee from it
- Patterns that have not shifted despite sustained self-work over 6 months or more
- The same relational dynamic repeating with different people, regardless of your awareness
Not all therapists are trained in attachment theory. Asking the five questions listed earlier in this article can help you evaluate whether a therapist understands attachment mechanics or is simply using the language without the clinical framework behind it.
Seeking therapy is not a sign that your self-work has failed. Many people find that self-awareness creates the foundation, and therapy provides the relational container where that awareness translates into felt, embodied change.
Readiness Self-Check (for all attachment styles)
- Rate on a 1–10 scale: How much distress do my attachment patterns cause in daily life?
- Rate on a 1–10 scale: How safe do I feel exploring these patterns alone?
- Rate on a 1–10 scale: How much have my patterns shifted from self-work alone?
- If your answer to question one is above 6, question two is below 5, or question three is below 3, professional support is likely to help
- Write down one specific pattern you would want to address in therapy—concreteness makes the step feel less overwhelming
For all attachment styles: noticing the impulse to skip this assessment or dismiss it as unnecessary is itself attachment-relevant data. Avoidant patterns may minimize the distress rating. Anxious patterns may inflate it. Disorganized patterns may find the scale itself confusing. Whatever you notice, it counts as useful information about where you are right now.
Frequently Asked Questions
Can therapy really change your attachment style?
Yes. A 2006 randomized controlled trial found that patients receiving Transference-Focused Psychotherapy shifted from insecure to secure attachment classification after 12 months. Meta-analyses confirm that improvements in attachment security during therapy coincide with better overall treatment outcomes.
How long does it take to change your attachment style in therapy?
Clinical consensus suggests one to two years of weekly therapy for meaningful attachment shift. The Levy et al. (2006) study showed classification changes at 12 months. Change unfolds through phases—alliance building, pattern recognition, corrective experiences, and integration—rather than arriving as a single breakthrough.
What type of therapy is best for attachment issues?
The best modality depends on your attachment style. EFT has the strongest evidence for couples and anxious attachment, with a meta-analytic effect size of 1.3. TFP is the only therapy proven in an RCT to change attachment classification. Disorganized attachment often benefits from trauma-informed approaches like somatic experiencing or EMDR.
Can you change your attachment style without therapy?
Secure relationships, security priming, and self-help tools can shift attachment patterns. Research shows 30 percent of adults change attachment classification over four years without intervention. Disorganized attachment and patterns rooted in significant trauma, however, typically benefit from professional support.
What is earned secure attachment?
Earned secure attachment describes people who developed insecure attachment in childhood but achieved secure functioning through therapy, relationships, or intentional work. About 14 percent of adults in one study were classified as earned secure. Research shows they demonstrate the same relationship outcomes as those who were always securely attached. Read more about what earned secure attachment means.
Does CBT work for attachment issues?
CBT can reduce attachment insecurity as a byproduct of treating anxiety or depression, but research suggests it may be less effective for avoidantly attached individuals who intellectualize without engaging emotionally. Adding relationally-oriented adjuncts or using attachment-focused CBT adaptations improves its effectiveness for attachment-specific change.
How does the therapeutic relationship change attachment?
The therapist serves as a temporary secure base—providing consistent attunement, co-regulation, and safe experiences of rupture and repair. Through repeated corrective attachment experiences, the client's internal working model gradually updates, and the security felt in therapy generalizes to other relationships.
Is attachment style permanent?
No. About 70 percent of adults retain the same classification over four years, but 30 percent shift categories without intervention. Fraley's prototype model suggests early patterns persist as defaults but remain open to updating through new relational experiences, therapy, and intentional practice.
Want to Go Deeper?
Meadow includes a structured assessment to help you understand your specific attachment patterns, followed by a 66-day program of daily practices designed to build earned security.
Start your free week →References
Randomized Controlled Trials and Meta-Analyses
Levy, K. N., Meehan, K. B., Kelly, K. M., Reynoso, J. S., Weber, M., Clarkin, J. F., & Kernberg, O. F. (2006). Change in attachment patterns and reflective function in a randomized control trial of transference-focused psychotherapy for borderline personality disorder. Journal of Consulting and Clinical Psychology, 74(6), 1027–1040.
Levy, K. N., Kivity, Y., Johnson, B. N., & Gooch, C. V. (2018). Adult attachment as a predictor and moderator of psychotherapy outcome: A meta-analysis. Journal of Clinical Psychology, 74(11), 1996–2013.
Bakermans-Kranenburg, M. J., van IJzendoorn, M. H., & Juffer, F. (2003). Less is more: Meta-analyses of sensitivity and attachment interventions in early childhood. Psychological Bulletin, 129(2), 195–215.
Pinquart, M., Feußner, C., & Ahnert, L. (2013). Meta-analytic evidence for stability in attachments from infancy to early adulthood. Attachment & Human Development, 15(2), 189–218.
Fraley, R. C. (2002). Attachment stability from infancy to adulthood: Meta-analysis and dynamic modeling of developmental mechanisms. Personality and Social Psychology Review, 6(2), 123–151.
Taylor, P., Rietzschel, J., Danquah, A., & Berry, K. (2020). Changes in attachment representations during psychological therapy: A meta-analysis. PMC.
Reviews and Theoretical Frameworks
Levy, K. N., & Johnson, B. N. (2018). Attachment and psychotherapy: Implications from empirical research. Canadian Psychology, 60(3), 166–176.
Mikulincer, M., & Shaver, P. R. (2020). Broaden-and-build effects of contextually boosting the sense of attachment security in adulthood. Current Directions in Psychological Science, 29(1), 22–26.
Feldman, R. (2017). The neurobiology of human attachments. Trends in Cognitive Sciences, 21(2), 80–99.
Porges, S. W. (2022). Polyvagal theory: A science of safety. Frontiers in Integrative Neuroscience, 16.
Schore, A. N. (2001). Effects of a secure attachment relationship on right brain development, affect regulation, and infant mental health. Infant Mental Health Journal, 22(1–2), 7–66.
Therapy-Specific Evidence
International Centre for Excellence in Emotionally Focused Therapy (ICEEFT). EFT research summaries and meta-analysis.
Wiebe, S. A., & Johnson, S. M. (2017). A review of the research in emotionally focused therapy for couples. Family Process, 55(3), 390–407.
CBT and attachment as moderator of outcome. PMC (2016).
Diamond, G. S., Kobak, R. R., Krauthamer Ewing, E. S., Levy, S. A., Herres, J. L., Russon, J. M., & Gallop, R. J. (2021). Attachment-based family therapy: A review of the empirical support. Family Process, 60(3), 725–741.
Neuroscience
Buchheim, A., Heinrichs, M., George, C., Pokorny, D., Koops, E., Henningsen, P., O'Connor, M. F., & Gündel, H. (2009). Oxytocin enhances the experience of attachment security. Psychoneuroendocrinology, 34(9), 1417–1422.
Koole, S. L., & Tschacher, W. (2022). Synchrony in psychotherapy: A review and an integrative framework for the therapeutic alliance. Frontiers in Human Neuroscience, 16.
Prevalence and Classification
Hazan, C., & Shaver, P. (1987). Romantic love conceptualized as an attachment process. Journal of Personality and Social Psychology, 52(3), 511–524.
Levine, A., & Heller, R. (2010). Attached: The new science of adult attachment and how it can help you find—and keep—love. TarcherPerigee.
Earned secure attachment prevalence study. PMC (2024).
This article is for educational purposes only and is not a substitute for professional mental health treatment. If you are experiencing significant distress related to your attachment patterns, please consult a licensed mental health professional. The exercises described here are intended as complements to—not replacements for—professional therapy when needed.
