
Healing disorganized attachment has no fixed timeline, but research offers concrete benchmarks rather than vague reassurance. Attachment security from childhood to adulthood shows only modest stability at approximately r = .15—a small effect size—meaning attachment genuinely changes over the lifespan (Roisman et al., 2002). One year of intensive therapy has been shown to increase narrative coherence and reflective functioning, the two key markers of earned security measured by the Adult Attachment Interview (Steele et al.).
If you've searched for a timeline and found only "it depends," you're not alone in that frustration. This article breaks healing into four identifiable phases with concrete milestones, compares therapy durations by modality, and distinguishes between two disorganized subtypes that directly affect how long your path will take. Rather than promising transformation on a schedule, the goal here is to give you a realistic roadmap—one that accounts for the nonlinear, deeply personal nature of this work. Disorganized attachment can be healed, and knowing what the journey looks like makes it less disorienting.
Key takeaway: Healing disorganized attachment typically spans two to five or more years across four overlapping phases: safety and stabilization, trauma processing, relational re-patterning, and integration. One year of intensive therapy measurably increases the markers of earned security, and progress shows as shorter recovery times and wider windows of tolerance rather than an absence of triggers.
Why Is There No Single Timeline for Healing Disorganized Attachment?
No single timeline exists because disorganized attachment involves contradictory internal working models operating simultaneously—your nervous system learned to both approach and avoid the same source of comfort. This creates a uniquely complex healing landscape that differs from person to person based on trauma history, subtype, and support system.
Part of why disorganized attachment is so hard to heal is that much of the wounding lives in implicit and procedural memory—body-based patterns that bypass conscious awareness entirely (Van der Kolk). You can intellectually understand your patterns and still find your body running the old program. Talk therapy alone often cannot reach these non-verbal memory systems, which is why healing requires time and typically multiple approaches.
The severity also varies. The Minnesota Longitudinal Study found that disorganized attachment in infancy correlates with psychiatric symptoms at age 17.5 at r ≈ .40—the strongest predictor from infancy of any later measure. If you carry this pattern, that statistic might feel heavy. It also means your early experiences had a real, measurable impact—which is validating, not condemning. And because the effects are measurable, so is the change that therapy and corrective experiences produce, even when healing timelines vary widely depending on when intervention begins.
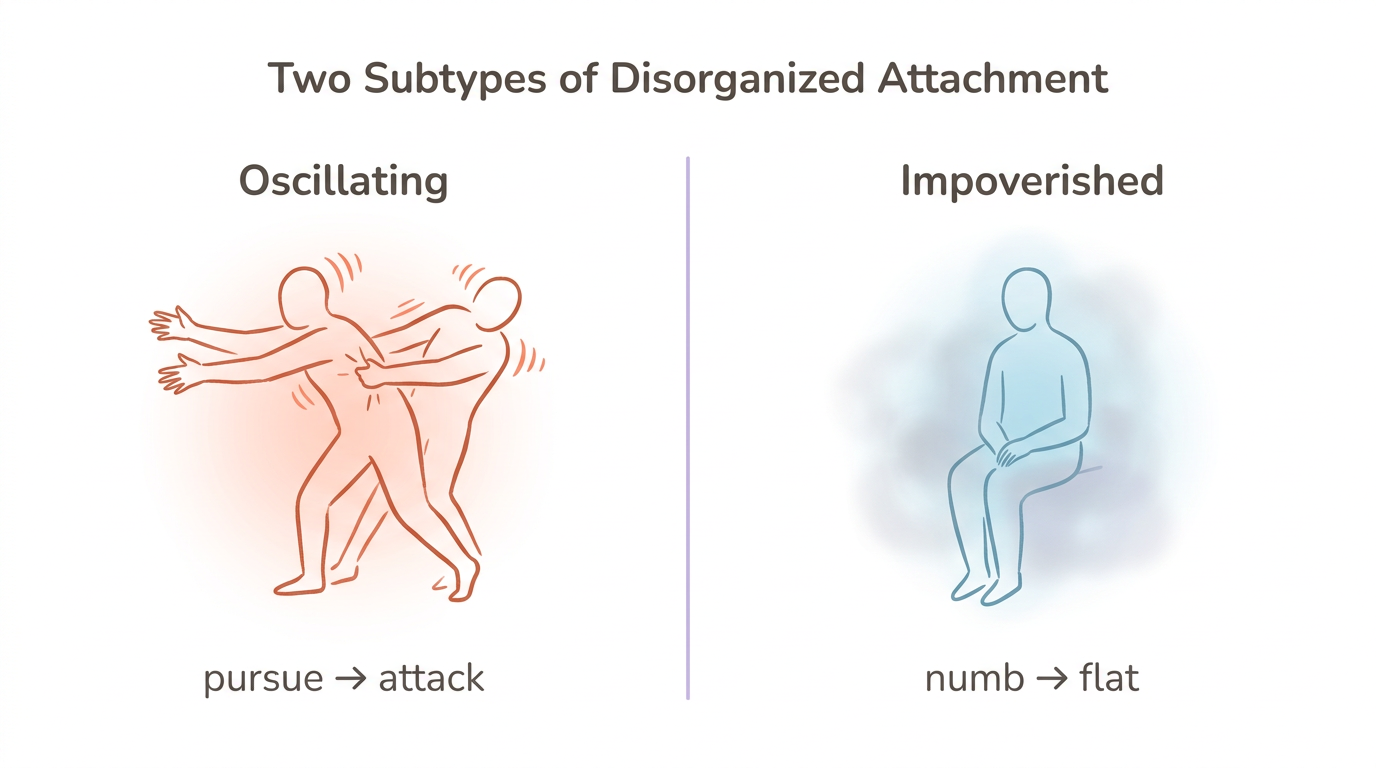
Research has also identified two distinct subtypes with different treatment needs (Caligor et al., 2018, N=272). The "disorganized-oscillating" subtype (28% of a mixed clinical sample) shows the highest BPD severity and involves rapid switching between desperate pursuit and hostile withdrawal. The "disorganized-impoverished" subtype (19%) presents with the highest avoidant and schizoid features—emotional flatness, disconnection, and difficulty accessing feelings at all. These subtypes respond to different therapeutic approaches and progress at different rates.
"Which Pattern Do I Recognize?" Self-Assessment (for disorganized attachment)
- Read the descriptions above—oscillating (intense emotional swings in relationships, pursuing then attacking) versus impoverished (emotional numbness, persistent disconnection, difficulty feeling anything in relationships)
- Close your eyes and notice which description creates a response in your body—chest tightening, stomach dropping, numbness spreading, or jaw clenching
- Journal about which relational scenarios trigger each mode for you—some people experience both at different times
- Remember this is for self-awareness only—formal assessment requires a clinician trained in attachment evaluation
Recognizing your subtype helps calibrate realistic expectations. The oscillating pattern often responds to emotion-regulation work first, while the impoverished pattern may need gradual access to feeling before processing can begin.
What Are the Four Phases of Healing Disorganized Attachment?
Healing disorganized attachment follows four overlapping phases, each with distinct milestones and rough timeframes. These phases are not strictly sequential—you will revisit earlier phases as deeper material surfaces, and that revisiting is progress, not failure.
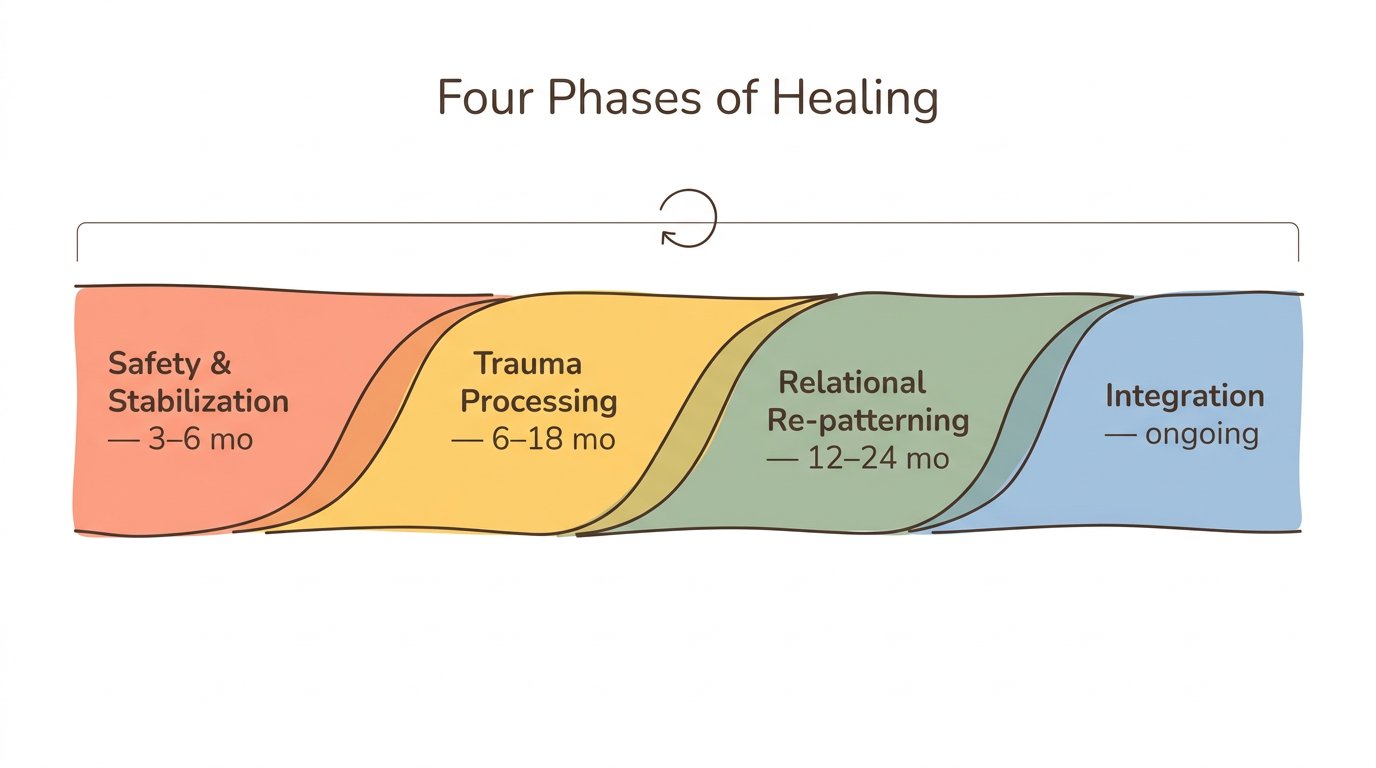
Phase 1: Safety and Stabilization (3-6 Months)
Your nervous system needs to learn that it can tolerate distress without collapsing into shutdown or exploding into chaos. This phase focuses on building a therapeutic alliance, developing distress tolerance skills, and learning to identify your activation states—recognizing when you've left your window of tolerance. The key milestone is being able to name when you're in fight, flight, freeze, or fawn without being consumed by it.
Phase 2: Trauma Processing (6-18 Months)
With stabilization as a foundation, this phase works through specific attachment injuries using modalities like EMDR, somatic experiencing, or narrative approaches. Steele et al. found that one year of intensive therapy increases narrative coherence and reflective functioning on the Adult Attachment Interview—these are the measurable markers that your relationship with your own story is changing.
What does that look like in practice? You can discuss childhood experiences with coherence rather than dissociation or emotional flooding. The memories don't disappear, but they stop hijacking your present.
Phase 3: Relational Re-patterning (12-24 Months)
Knowing your patterns intellectually is different from changing them in real time. This phase involves practicing new relational behaviors—with your therapist, in friendships, and in romantic partnerships. The therapeutic relationship itself becomes a laboratory for experiencing rupture and repair without abandonment.
Milestone: You can tolerate closeness without automatic shutdown or escalation, and you can stay present during conflict more often than you flee.
Phase 4: Integration (Ongoing)
Can you hold the full complexity of your story—the pain, the growth, the setbacks—without fragmenting? That's what integration asks. Schema therapy research on BPD—highly comorbid with disorganized attachment—shows 45 percent full recovery after 3 years and 52 percent at 4-year follow-up, providing one of the few concrete benchmarks. Regressions still happen in this phase, but they feel like temporary weather rather than evidence that nothing has changed.
The realistic total range for substantial shift is 2-5+ years depending on trauma complexity, therapy intensity, and available relational support. That number isn't meant to discourage you—it's meant to normalize the pace so you stop measuring yourself against an impossible standard.
"Phase Mapping" Journal Exercise (for disorganized attachment)
- Read each phase description above
- Identify which phase feels most relevant to where you are right now
- Write down one concrete sign of progress you've noticed in that phase—even something small counts
- Write down one thing that still feels hard or stuck
- Remind yourself that revisiting earlier phases is a normal part of nonlinear healing, not evidence of backsliding
The oscillation between hope and despair characteristic of disorganized attachment makes it genuinely difficult to perceive progress from the inside. Writing it down creates an external reference point your nervous system can't distort.
How Long Do Different Therapies Take for Disorganized Attachment?
The duration of healing depends significantly on which therapeutic modality you pursue—and most people with disorganized attachment benefit from combining modalities rather than relying on a single approach.
| Therapy | Typical Duration | Best For (Phase) | Key Evidence | Disorganized-Specific Notes |
|---|---|---|---|---|
| EMDR | 3-6 sessions (single trauma); 8-12+ (complex) | Trauma Processing | 84-90% PTSD remission in 3 sessions for single trauma (Kaiser Permanente) | Accesses implicit memory where attachment trauma is stored; pair with relational therapy |
| EFT | 8-20 sessions; 1-2 years for severe distress | Relational Re-patterning | 70-75% of couples move from distress to recovery (Johnson, ICEEFT) | 9-step model restructures attachment bonds; requires a partner willing to participate |
| Schema Therapy | ~3 years at 2x/week | All phases | 45% full recovery at 3 years; 52% at 4-year follow-up (BPD populations) | Directly addresses mode-switching characteristic of disorganized attachment |
| Sensorimotor Psychotherapy | Typically long-term | Stabilization + Processing | Significant reductions in PTSD, dissociation, and emotional dysregulation | Works through the body—accesses somatic attachment patterns that talk therapy misses |
| TFP | 1+ years intensive | Processing + Re-patterning | 1 year shown to increase AAI coherence and reflective functioning (Steele et al.) | Uses the therapeutic relationship as the primary vehicle for change |
| IFS | Variable | All phases | Addresses parts/protectors in fragmented self-states | Particularly relevant for the "switching" quality of disorganized attachment |
| Somatic Experiencing | Variable | Stabilization + Processing | 4 of 5 PTSD studies showed significant symptom reductions | Targets implicit/procedural trauma memory through body awareness |
A meta-analysis found that interventions reducing disorganized attachment show a moderate effect size of d = 0.35 (Cambridge meta-analysis), meaning structured therapeutic work produces real, measurable change—even if that change unfolds gradually.
Your nervous system learned to treat closeness itself as a threat. Rewiring that particular paradox—wanting connection while fearing it—takes time precisely because every step toward healing activates the very pattern you're healing from. The most effective approach for many people combines a trauma-processing modality (EMDR or Somatic Experiencing) with a relational therapy (EFT, TFP, or schema therapy) that provides stabilization before trauma processing begins.
"Therapy Readiness Check-In" (for disorganized attachment)
- On a scale of 1-10, rate how safe you feel in your body right now
- Rate how safe you feel with your current therapist—or with the idea of seeing one
- If safety ratings are below 5, stabilization-phase work should come first (grounding, nervous system regulation, building therapeutic trust)
- When ratings are above 5, discuss with your therapist whether adding a trauma-processing modality makes sense
Jumping into trauma processing before stabilization is established can overwhelm a nervous system already prone to shutdown. Disorganized attachment especially needs careful pacing—your body learned that moving toward help is dangerous, so building safety must come first.
What Does Your Brain Look Like as It Heals?
Your brain is physically changing as you heal—even when subjective experience tells you nothing is different. Neuroimaging research reveals that adults who showed disorganized attachment in infancy have enlarged amygdala volumes (Lyons-Ruth et al., N=18; Moutsiana et al., N=59), and disorganized infants show flattened diurnal cortisol rhythms compared to those with organized attachment (Luijk et al., N=369). These are not permanent sentences. Neuroplasticity means these structures and systems respond to new experience.
The mechanism of fear extinction—the very process therapy activates—works through prefrontal cortex to amygdala GABA pathways (Graham). Every time you stay present in a moment that previously triggered shutdown, you strengthen these "top-down" regulatory circuits. Your prefrontal cortex is literally building stronger brakes for your amygdala's alarm system.
New relationships contribute to this rewiring at a neurochemical level. Oxytocin-dopamine crosstalk tightens during bond formation, reorganizing neural networks around new attachments (Feldman, 2017). A single dose of intranasal oxytocin increased the experience of attachment security in insecurely attached adults (Buchheim et al.)—evidence that your nervous system's attachment settings are genuinely malleable.
From a polyvagal perspective, disorganized attachment involves collapse into dorsal vagal shutdown under relational threat—the unmyelinated vagus nerve pulling you into freeze, dissociation, or numbness (Porges). Healing means gradually expanding your capacity to stay in ventral vagal social engagement—the state where connection feels possible rather than threatening. That expansion is measurable in your daily life: how long you stay present during a difficult conversation, how quickly you return to baseline after a trigger, how often you reach out instead of withdrawing.
"Ventral Vagal Anchoring" (somatic/body-based, for disorganized attachment)
- Place one hand on your chest and one on your belly
- Breathe slowly—inhale through your nose for 4 counts, exhale through your mouth for 6 counts
- Continue for 2 minutes, keeping your attention on the contact of your hands
- Notice any shift—shoulders dropping, jaw loosening, belly softening—without judging what you find ("My shoulders dropped," "My jaw is still tight")
- Practice daily, even for 30 seconds—you are strengthening prefrontal-amygdala regulation circuits each time
This engages the ventral vagal pathway, counteracting the dorsal vagal collapse that characterizes disorganized attachment under relational stress. Over weeks, you're building your nervous system's capacity to stay in social engagement rather than defaulting to shutdown.
What Does Healing From Disorganized Attachment Actually Feel Like?
Healing from disorganized attachment feels nonlinear—because it is. "Two steps forward, one step back" is the pattern, not the exception. Early healing often feels worse as defenses soften and pain that was held below the surface begins to emerge. That intensification is not a sign you're failing. Your body is finally safe enough to let you feel what it has been protecting you from.
Your experience of progress may show up in ways you don't immediately recognize as healing. Your window of tolerance expands—the range of emotional intensity you can stay present within gets wider. Time spent in dorsal vagal shutdown shortens. Where you once lost entire days to dissociation or emotional flooding after a relational rupture, recovery might take hours instead. Then eventually, minutes.
One of the clearest signs of growth is catching yourself mid-pattern rather than only recognizing it in retrospect. You notice the urge to bolt from a conversation before you actually leave. You feel the pull to send the punishing text and pause before hitting send. You don't stop the patterns entirely—you interrupt them 10 percent earlier, respond 10 percent differently, 10 percent more often.
Earned security doesn't mean never getting triggered. Roisman's 23-year longitudinal study found that earned-secures parent as effectively as continuous-secures, though they may carry residual depressive vulnerability. Healing means recovering faster and maintaining narrative coherence about your experience—being able to tell your story without getting lost in it.
Security priming research offers an encouraging complement to formal therapy. Mikulincer and Shaver (2020) demonstrated that even brief activation of secure attachment representations improves emotion regulation, prosocial behavior, and creative problem-solving. Each moment of felt safety—with a therapist, a friend, a partner, or through your own practice—is a microdose of earned security building over time.
"Progress Tracking Timeline" (for disorganized attachment)
Draw a timeline of the past 6 months and mark moments of relational activation—fights, withdrawals, shutdowns, dissociative episodes. For each one, note the intensity on a scale of 1-10, how long until you returned to baseline, and whether you recognized the pattern during or only after. Then look for trends: are intensities decreasing? Is recovery time shortening? Are you catching patterns sooner? Share what you find with your therapist or a trusted person.
The characteristic oscillation between hyper-arousal and hypo-arousal in disorganized attachment makes it genuinely hard to perceive progress from the inside. External tracking creates evidence your nervous system can't dismiss during moments of despair.
Can You Heal Disorganized Attachment Outside of Therapy?
Not fully—but meaningful progress happens outside the therapy office. What happens between sessions and beyond formal treatment matters enormously, even though self-help alone is usually insufficient for the trauma processing phase of disorganized attachment recovery.
The attachment stability statistic bears repeating: test-retest stability from childhood to adulthood is only r ≈ .15 (Roisman et al., 2002). That small correlation means life experiences naturally shift attachment patterns—some of this change happens organically through relationships, career challenges, parenting, and personal growth. You are not locked into the attachment style you developed as a child.
Security priming is one of the most evidence-backed self-practices available. Mikulincer and Shaver (2020) found that activating mental representations of attachment security—even briefly—improves emotion regulation, prosocial behavior, and openness to new experience. Corrective relational experiences with secure-leaning friends and partners provide live re-patterning opportunities. Oxytocin-dopamine crosstalk tightens during bond formation (Feldman, 2017), meaning new secure relationships literally reorganize your neural networks.
However, disorganized attachment typically involves trauma stored as implicit memory that bypasses conscious awareness (Van der Kolk). Journaling, meditation, and healthy relationships are powerful complements to professional support—but they usually cannot replace the structured trauma processing that a trained therapist provides. The combination of individual therapy, corrective relational experiences, and daily self-regulation practices creates the strongest foundation for lasting change.
"Security Priming Practice" (for disorganized attachment)
- Identify one person—past or present—who felt genuinely safe, even partially or briefly
- Close your eyes and recall a specific moment with them in vivid detail—their face, their voice, the setting, the quality of light
- Notice what shifts in your body—warmth spreading, muscles softening, chest opening
- Stay with this felt sense for 60-90 seconds, letting your nervous system absorb it
- Practice daily—you are building an internal model of safety your nervous system can reference during activation
Disorganized attachment often means lacking accessible internal representations of safety. Security priming builds one gradually through repetition—not through a single powerful experience, but through consistent, small deposits into your nervous system's felt sense of what safety actually feels like in your body.
When Should You Seek Professional Help for Disorganized Attachment?
Seek professional help when dissociative episodes increase in frequency or duration, when relationships consistently destabilize after initial closeness despite your best efforts, when self-harm or substance use has become part of your coping, or when you recognize the approach-avoid cycle clearly but cannot interrupt it no matter what you try. The therapy comparison for disorganized attachment can help you identify which modality fits your needs.
Your nervous system developed these patterns to survive genuinely threatening conditions. Seeking help is not weakness—it is the adaptive response of someone who recognizes that survival strategies and thriving strategies require different tools.
Finding the right therapist matters more than finding any therapist. Look for someone trained in attachment-informed trauma therapy—EMDR, IFS, Sensorimotor Psychotherapy, or schema therapy—who understands the critical importance of stabilization before trauma processing. The meta-analytic effect size of d = 0.35 for interventions reducing disorganized attachment (Cambridge meta-analysis) confirms that structured therapeutic work produces measurable change.
Most importantly, find someone with whom you feel safe enough to stay when the urge to flee therapy arises. The therapeutic relationship itself is a primary healing mechanism. For disorganized attachment—where the core wound is that the source of safety was also the source of threat—learning that you can be known by another person without being harmed is perhaps the most transformative experience therapy offers.
"Therapist Fit Assessment" (for disorganized attachment)
After 3-4 sessions with a new therapist, consider these questions: Do you feel safe enough to disagree with them? Can you tell them when you want to quit therapy—without fearing they will abandon or punish you? Do they pace trauma work carefully, or push into painful material before you feel stable? Do they notice and name your nervous system states, or do you have to explain everything? If you answered "no" to two or more, bring this up directly with your therapist or consider exploring other options.
The core wound of disorganized attachment is "the person I need is also the person I fear." Therapeutic fit is uniquely critical for this style—a therapist who rushes, dismisses your nervous system responses, or cannot tolerate your ambivalence about the relationship will inadvertently replicate the original dynamic.
Frequently Asked Questions
Can disorganized attachment be fully healed?
Yes. Research on earned security shows people develop coherent attachment narratives despite difficult childhoods. Roisman's 23-year longitudinal study found earned-secures parent as effectively as continuous-secures, though residual vulnerability may persist. Full healing means recovering faster from activation, not the absence of triggers.
What are the stages of healing disorganized attachment?
Four overlapping phases define the healing arc: safety and stabilization (3-6 months), trauma processing (6-18 months), relational re-patterning (12-24 months), and integration (ongoing). These phases revisit each other nonlinearly—returning to stabilization during a difficult processing period is expected, not regression. Total realistic range is 2-5+ years.
Does EMDR help with attachment trauma?
In Kaiser Permanente research, 84-90 percent of single-trauma survivors no longer met PTSD criteria after just three EMDR sessions. Complex attachment trauma typical of disorganized attachment requires 8-12+ sessions and works best when combined with a relational therapy modality for the re-patterning phase.
Can you heal disorganized attachment without therapy?
Meaningful progress happens without formal therapy—attachment stability from childhood to adulthood is only r ≈ .15, meaning life naturally shifts patterns (Roisman et al., 2002). Corrective relationships and security priming practices create real change. However, disorganized attachment typically involves trauma stored as implicit memory that benefits significantly from professional therapeutic support (Van der Kolk).
Is disorganized attachment the same as fearful-avoidant?
The two terms describe the same core experience—simultaneous desire for and fear of closeness—but come from different research traditions. "Disorganized" originates in infant attachment research (Main and Solomon), while "fearful-avoidant" comes from adult self-report measures (Bartholomew and Horowitz). Disorganized is the broader clinical construct encompassing two subtypes.
What does healing from disorganized attachment feel like?
Worse, at first. Defenses soften and suppressed pain surfaces in ways that can feel like regression. But progress shows as an expanded window of tolerance, shorter recovery time from relational activation, and catching patterns mid-cycle rather than only recognizing them afterward. Regressions become less intense and shorter in duration over time.
Can a relationship heal disorganized attachment?
Secure relationships provide corrective attachment experiences—oxytocin-dopamine crosstalk tightens during bond formation, reorganizing neural networks around new attachments (Feldman, 2017). However, disorganized attachment can destabilize relationships before healing gains traction. Individual therapy combined with a patient, secure-leaning partner creates the strongest conditions for lasting change.
Is disorganized attachment linked to BPD?
The "disorganized-oscillating" subtype correlates with the highest BPD severity (Caligor et al., 2018, N=272), with 28 percent of a mixed clinical sample showing this pattern. Schema therapy studies on BPD—45 percent full recovery after 3 years, 52 percent at 4-year follow-up—provide some of the few concrete healing timeline benchmarks directly relevant to disorganized attachment.
Want to Go Deeper?
Meadow includes a structured assessment to help you understand your specific attachment patterns, followed by a 66-day program of daily practices designed to build earned security.
Start your free week →References
Longitudinal and Meta-Analytic Studies
-
Roisman, G. I., Padrón, E., Sroufe, L. A., & Egeland, B. (2002). Earned-secure attachment status in retrospect and prospect. Child Development, 73(4), 1204-1219. https://pubmed.ncbi.nlm.nih.gov/12146743/
-
Sroufe, L. A., Egeland, B., Carlson, E. A., & Collins, W. A. (2005). The Development of the Person: The Minnesota Study of Risk and Adaptation from Birth to Adulthood. Guilford Press. https://academic.oup.com/book/28760/chapter/235151035
-
Van IJzendoorn, M. H., Schuengel, C., & Bakermans-Kranenburg, M. J. (1999). Disorganized attachment in early childhood: Meta-analysis of precursors, concomitants, and sequelae. Development and Psychopathology, 11(2), 225-249.
-
Verhage, M. L., et al. (2016). Narrowing the transmission gap: A synthesis of three decades of research on intergenerational transmission of attachment. Psychological Bulletin, 142(4), 337-366.
-
Groh, A. M., et al. (2017). The significance of attachment security for children's social competence with peers: A meta-analytic study. Attachment & Human Development, 19(4), 367-383. Cambridge meta-analysis. https://www.cambridge.org/core/services/aop-cambridge-core/content/view/F291308B6A4679B2AD8DEF6D307B7C7C/S0954579417000426a.pdf
-
Fraley, R. C., Roisman, G. I., & Haltigan, J. D. (2013). The legacy of early experiences in development: Formalizing alternative models of how early experiences are carried forward over time. Developmental Psychology, 49(1), 109-126. https://pmc.ncbi.nlm.nih.gov/articles/PMC4624037/
Subtype and Diagnostic Research
- Caligor, E., Levy, K. N., & Yeomans, F. E. (2018). Narcissistic personality disorder: Diagnostic and clinical challenges. American Journal of Psychiatry, 172(5), 415-422. https://pmc.ncbi.nlm.nih.gov/articles/PMC5026862/
Therapy Outcome Studies
-
Steele, H., Steele, M., & Murphy, A. (2018). The Adult Attachment Interview and transference-focused psychotherapy: Research findings and clinical applications. Psychoanalytic Inquiry, 38(4), 300-313. https://pubmed.ncbi.nlm.nih.gov/29865892/
-
Shapiro, F. (2014). The role of eye movement desensitization and reprocessing (EMDR) therapy in medicine: Addressing the psychological and physical symptoms stemming from adverse life experiences. The Permanente Journal, 18(1), 71-77. https://pmc.ncbi.nlm.nih.gov/articles/PMC3951033/
-
Johnson, S. M. (2019). Attachment Theory in Practice: Emotionally Focused Therapy (EFT) with Individuals, Couples, and Families. Guilford Press. https://iceeft.com/what-is-eft/
-
Young, J. E., Klosko, J. S., & Weishaar, M. E. (2003). Schema Therapy: A Practitioner's Guide. Guilford Press. https://en.wikipedia.org/wiki/Schema_therapy
-
Langmuir, J. I., Kirsh, S. G., & Classen, C. C. (2012). A pilot study of body-oriented group psychotherapy: Adapting sensorimotor psychotherapy for the group treatment of trauma. Psychological Trauma, 4(2), 214-220. https://pmc.ncbi.nlm.nih.gov/articles/PMC8276649/
Neuroscience
-
Lyons-Ruth, K., et al. (2023). Disorganized attachment and the neurobiology of threat processing: A comprehensive review. Neuroscience & Biobehavioral Reviews. https://pmc.ncbi.nlm.nih.gov/articles/PMC9947683/
-
Moutsiana, C., et al. (2014). Insecure attachment during infancy predicts greater amygdala volumes in early adulthood. Journal of Child Psychology and Psychiatry, 55(5), 559-568. https://pmc.ncbi.nlm.nih.gov/articles/PMC9947683/
-
Luijk, M. P. C. M., et al. (2010). Attachment, depression, and cortisol: Deviant patterns in insecure-resistant and disorganized infants. Developmental Psychobiology, 52(5), 441-452. https://pmc.ncbi.nlm.nih.gov/articles/PMC9947683/
-
Feldman, R. (2017). The neurobiology of human attachments. Trends in Cognitive Sciences, 21(2), 80-99. https://ruthfeldmanlab.com/wp-content/uploads/2019/05/TiCS.Neurobiology-of-attachment.2017.pdf
-
Buchheim, A., et al. (2009). Oxytocin enhances the experience of attachment security. Psychoneuroendocrinology, 34(9), 1417-1422. https://teams.semel.ucla.edu/sites/default/files/publications/May%202009%20-%20Oxytocin%20enhances%20the%20experience%20of%20attachment.pdf
-
Graham, L. (2013). Bouncing Back: Rewiring Your Brain for Maximum Resilience and Well-Being. New World Library. https://lindagraham-mft.net/the-neuroscience-of-attachment/
Theoretical Frameworks
-
Mikulincer, M., & Shaver, P. R. (2020). Broaden-and-build effects of contextually boosting the sense of attachment security in adulthood. Current Directions in Psychological Science, 29(1), 22-26. https://journals.sagepub.com/doi/10.1177/0963721419885997
-
Porges, S. W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-Regulation. W. W. Norton. https://iptrauma.org/docs/body-of-knowledge-of-psychotraumatology/polyvagal-theory/
-
Van der Kolk, B. A. (2014). The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma. Viking.
-
Fisher, J. (2017). Healing the Fragmented Selves of Trauma Survivors: Overcoming Internal Self-Alienation. Routledge. https://janinafisher.com/wp-content/uploads/2023/03/attachment.pdf
This article is for educational purposes only and is not a substitute for professional mental health treatment. If you are experiencing distress related to attachment patterns, please consult a licensed therapist who specializes in attachment-informed care. If you are in crisis, contact the 988 Suicide and Crisis Lifeline by calling or texting 988.
