
EMDR (Eye Movement Desensitization and Reprocessing) is a therapy that uses bilateral stimulation to help the brain reprocess traumatic memories. In a study of 20 adults assessed with the Adult Attachment Interview, Civilotti et al. (2019) found significant shifts from insecure and unresolved attachment classifications to secure after EMDR treatment.
EMDR is one of the most well-researched trauma therapies available—recommended by the WHO, APA, and NICE, with over 30 randomized controlled trials supporting its use for PTSD (EMDRIA). Yet most of that evidence addresses single-incident trauma, not the relational wounds that shape attachment. If you're wondering whether EMDR can reach the deeper, earlier, implicit memories driving your attachment patterns, the honest answer is nuanced. The research is promising but still early, and how EMDR is applied matters as much as whether it's applied at all.
Key takeaway: EMDR shows promising preliminary evidence for shifting attachment patterns from insecure to secure, though research remains limited to small pilot studies. Standard EMDR works best for single-incident trauma, while attachment-focused EMDR was specifically designed for the relational wounds that shape insecure attachment. The approach matters as much as the modality itself.
What does EMDR actually do to traumatic memories?
EMDR transforms how traumatic memories are stored—the event remains but loses its emotional charge. Using bilateral stimulation—eye movements, taps, or tones alternating between left and right sides of the body—EMDR guides the brain through Shapiro's 8-phase protocol. During processing, the traumatic memory enters a labile state through a process called memory reconsolidation. You can recall the event without being overwhelmed by it.
This process appears to activate neural patterns similar to REM sleep, when your brain naturally consolidates and processes emotional experiences. That's part of why EMDR can sometimes work faster than talk therapy for discrete traumatic events. If a memory from years ago still floods your body as though it's happening now, that's your nervous system holding unfinished processing. EMDR lets your nervous system complete that processing—finishing what was interrupted during the original experience.
The APA, WHO, and NICE all recommend EMDR for PTSD, and over 30 randomized controlled trials support its efficacy (EMDRIA). A 2024 meta-analysis found a Hedges' g of 0.75 across 25 studies and 1,042 participants for depression symptoms as well.
Before reading further, try this brief exercise to connect with the somatic awareness that EMDR builds on.
Body Scan Awareness Check-In (for all attachment styles)
Close your eyes and recall a mildly uncomfortable relational moment—not the most painful, just one that carries a small charge. Scan slowly from the top of your head down to your feet, noticing where tension, tightness, or numbness appears—your jaw, chest, stomach, hands. Place one hand on that spot and take three slow breaths. Notice any shift in the sensation, even slight.
This introduces the body awareness EMDR relies on. Attachment patterns live in the body as much as the mind—your nervous system holds relational memories even when your conscious mind has moved on.
Why does standard EMDR struggle with attachment trauma?
A car accident, an assault, a single overwhelming event—standard EMDR was built for these discrete incidents. Attachment trauma is fundamentally different. It's chronic relational trauma built from thousands of daily micro-experiences of inconsistency, neglect, or frightening caregiving. There's often no single target memory because the wound wasn't one moment but an entire relational environment.
Three specific problems emerge when standard EMDR meets attachment wounds. First, clients with insecure attachment may struggle to form the therapeutic bond that EMDR requires—the very capacity that needs healing is the one the treatment depends on. Second, anxious or disorganized clients may become flooded by intense affect during processing, pushed outside their window of tolerance. Third, attachment trauma is stored as implicit memory—body sensations, procedural responses, felt senses that formed before language developed. Standard EMDR's reliance on identifying a specific target image and negative cognition doesn't map neatly onto these pre-verbal experiences.
Wesselmann et al. (2012) noted in their literature review that while evidence for EMDR's impact on attachment is "promising," it remains "preliminary"—in part because the standard protocol wasn't built for this kind of wound.
Window of Tolerance Self-Check (for anxious and avoidant attachment)
- Rate your current distress on a scale of 0 to 10
- Identify your signs of hyperarousal—racing heart, restlessness, inability to stop thinking
- Identify your signs of hypoarousal—numbness, fogginess, feeling disconnected or "checked out"
- Ask yourself: under relational stress, which direction do I tend to go?
- Write down your answer—this self-knowledge is essential information for any therapist you work with
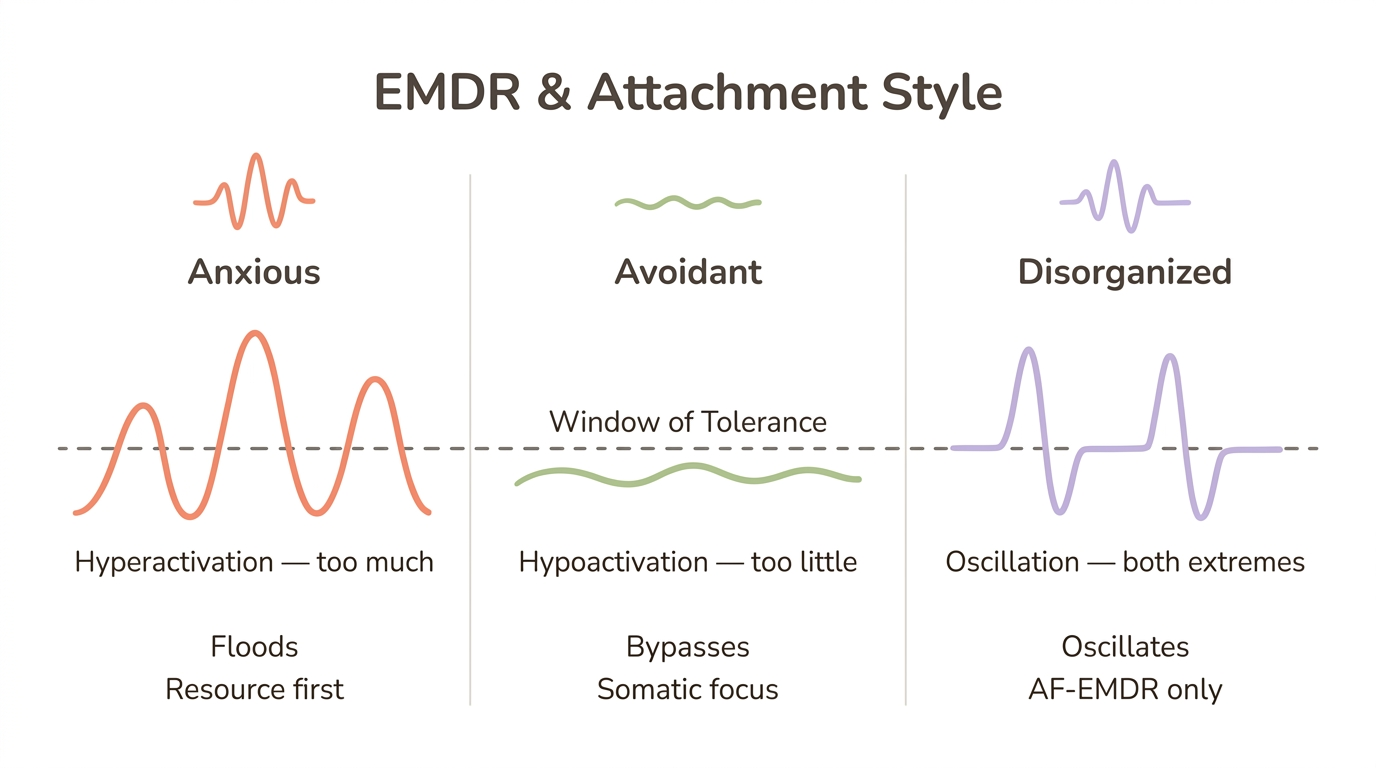
This exercise reveals why standard EMDR can push attachment-wounded clients outside their processing capacity. Anxious attachment typically correlates with hyperarousal (the nervous system stuck in "too much"), while avoidant attachment often correlates with hypoarousal (the nervous system in "too little"). Your therapist needs to know your pattern to pace EMDR appropriately.
What is attachment-focused EMDR and how is it different?
If standard EMDR struggles with relational trauma, what does a modified version actually look like? Laurel Parnell (2008) developed attachment-focused EMDR (AF-EMDR) specifically to address these limitations. Where standard EMDR assumes a client can tolerate intense processing relatively quickly, AF-EMDR builds resources first so the nervous system can handle what comes up.
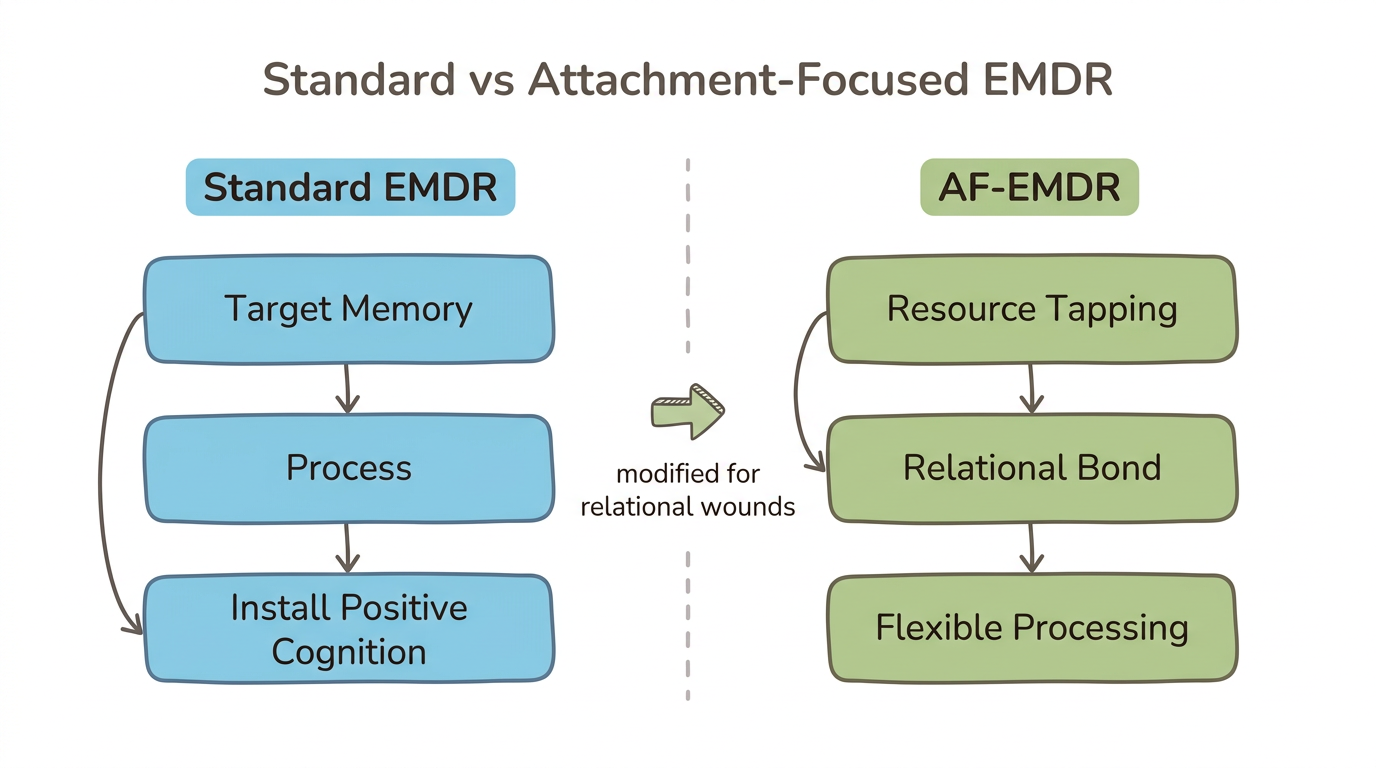
The key modifications include resource tapping—bilateral stimulation paired with positive imagery to create an internal sense of safety before any trauma processing begins. AF-EMDR also uses a modified Phase 3 that doesn't require a Positive Cognition, making entry into processing more flexible for clients whose attachment wounds don't fit neat cognitive categories. Integrated talk therapy and a strong emphasis on the therapeutic relationship as a corrective attachment experience round out the approach.
Parnell organized AF-EMDR around five core principles:
- Safety — establishing internal and external safety before any processing
- Therapeutic relationship — the therapist-client bond is itself a vehicle for attachment repair
- Client-centered approach — following the client's pace rather than a rigid protocol
- Resource tapping — building positive internal resources through bilateral stimulation before processing negative material
- Modified EMDR protocol — adapting the standard phases to fit relational trauma's non-linear nature
For those with disorganized attachment, AF-EMDR's emphasis on resourcing and relational safety is especially important. The standard protocol's directive structure can feel overwhelming when your nervous system learned that closeness itself is the threat.
Resource Tapping Preview (for all attachment styles, especially disorganized)
- Think of a person, place, animal, or memory where you felt genuinely safe—even briefly
- Hold that image in your mind and notice what sensations arise in your body
- Alternate tapping your knees left-right slowly for 30 seconds while holding the image
- Pause and notice—has the positive sensation strengthened, stayed the same, or shifted?
- If it strengthened, repeat for another 30 seconds to deepen the resource
This is a simplified version of the resourcing phase that makes AF-EMDR safer for attachment-wounded clients. You're pairing bilateral stimulation with positive experience, building an internal secure base your nervous system can return to during difficult processing. This works for attachment specifically because it creates the felt sense of safety that inconsistent caregiving never provided.
Can EMDR actually change your attachment style?
Preliminary but promising—that's the most honest summary of where the evidence stands. Three studies have directly measured attachment change following EMDR, and all found positive results, but all had small sample sizes.
Civilotti et al. (2019) assessed 20 adult women using the Adult Attachment Interview before and after EMDR treatment. They found significant shifts from dismissing, preoccupied, and unresolved classifications toward secure. Participants also showed increased narrative coherence and reflective functioning—both markers of earned secure attachment.
Wesselmann and Potter (2009) published three case studies of adults with insecure or disorganized attachment who received 10 to 15 EMDR sessions over approximately one year. All three participants showed positive changes in attachment status on the AAI and reported improvements in emotional functioning and relationships.
Barazzone et al. (2023) conducted a pilot study with 18 participants, most of whom had fearful attachment. After an average of 15 EMDR sessions, they measured significant reduction in fearful attachment scores and significant decrease in dismissive attachment (d = 0.42).
The critical caveat: no large-scale RCT specifically examining EMDR's effect on attachment security exists yet. These studies involved 3 to 20 participants. The direction of the evidence is encouraging, and the neurobiological mechanisms make theoretical sense, but the research is still in its early stages. If someone tells you EMDR is "proven" to change attachment, that's overstating what the science currently supports. If someone tells you it can't, they're ignoring promising preliminary data. Can therapy change your attachment style? The evidence says yes—EMDR may be one pathway among several.
Narrative Coherence Reflection (for all attachment styles, especially avoidant and disorganized)
Write 3 to 4 sentences about your childhood relationship with your primary caregiver—whatever comes naturally. Read it back slowly and notice: does it feel fragmented? Overly brief? Contradictory? Notice where you minimize ("it wasn't that bad"), idealize ("everything was fine"), or get pulled into unresolved emotion mid-sentence. There's no wrong answer—you're observing your narrative pattern, not fixing it.
The Adult Attachment Interview measures exactly this: how coherently you can tell the story of your early relationships. EMDR appears to increase this coherence. Avoidant attachment often shows in brief, idealized narratives that lack detail. Disorganized attachment often shows in fragmented stories that shift suddenly in tone. Noticing your pattern is the first step toward understanding what EMDR would be working with.
What happens in your brain during EMDR that helps attachment?
You might wonder why a therapy designed for PTSD could reach something as deep as attachment. The answer shows up on brain scans. EMDR produces measurable changes in brain function that map directly onto the neural patterns disrupted by insecure attachment.
Amygdala calming
fMRI studies show that EMDR decreases amygdala activation when processing traumatic memories, reducing the fear and threat response. This matters for attachment because insecure attachment is associated with amygdala hyperreactivity to relational cues. Your nervous system fires alarm signals at a partner's tone shift or delayed text response. Those alarm signals made sense when you were small and your caregiver's tone shift meant something was about to go wrong. EMDR appears to dial down that reactivity at its neural source. For more on how attachment shapes your nervous system's threat detection, see how attachment style affects your nervous system.
Prefrontal cortex strengthening
EMDR increases prefrontal cortex activity, enhancing emotional regulation and cognitive control—both capacities that insecure attachment undermines. This neuroplasticity means the brain isn't just processing old memories but building new regulatory capacity. You're not just resolving the past; your brain is getting better at managing the present.
Network-level rebalancing
Attachment trauma disrupts three major brain networks: the default mode network (self-referential processing), the salience network (threat detection), and the central executive network (cognitive control). EMDR restores network-level rebalancing across all three, potentially explaining why it can shift something as pervasive as attachment—which touches self-perception, threat sensitivity, and executive functioning simultaneously. Research on brain connectivity changes supports these structural shifts (EMDRIA).
Morphometric studies have also identified hippocampal and limbic structural changes following EMDR, suggesting actual neuroplasticity rather than just temporary functional shifts. These findings align with the broader research on healing your nervous system from attachment trauma.
Bilateral Grounding Sequence (for anxious and disorganized attachment)
Cross your arms over your chest in a "butterfly hug" position, fingertips resting on your shoulders. Alternate tapping your shoulders slowly—left, right, left, right—at a pace that feels calming. While tapping, simply notice sensations in your body without trying to change anything. Continue for 60 seconds, then pause with your hands in your lap and observe any shift—even subtle—in your level of activation or calm.
This gives you a felt sense of bilateral stimulation's effect on your nervous system. For anxious attachment, this can interrupt the hyperactivation cycle that drives reassurance-seeking. For disorganized attachment, the rhythmic, predictable alternation provides the kind of structured, safe sensory input your nervous system rarely experienced in early relationships.
How does EMDR work differently for each attachment style?
EMDR doesn't affect every attachment style the same way, and your therapist's approach should reflect your specific pattern. This is where attachment-informed EMDR diverges most from generic trauma processing.
Anxious attachment
If you have anxious attachment, your nervous system runs hot under relational threat. During EMDR processing, this hyperactivation can flood the system—emotions intensify rather than resolve. You may need an extended resourcing phase before any trauma processing begins. The therapeutic relationship itself may trigger attachment activation: wanting more sessions, fearing the therapist will leave, reading into scheduling changes. AF-EMDR's emphasis on the therapeutic bond as a corrective experience is especially valuable here. Your body learned that connection means anxiety. EMDR can help it learn something different—but only if the pace respects your nervous system's sensitivity.
Avoidant attachment
You're in a session, recalling a memory of your parent's emotional absence, and you hear yourself saying "It wasn't a big deal, honestly." That familiar impulse to intellectualize shows up during bilateral stimulation too. Avoidant clients may process memories at a cognitive level while remaining disconnected from the body and emotion—a form of emotional bypassing that looks like progress but doesn't produce lasting change. You might minimize memories, rush through processing, or report feeling "fine" when your body is clearly holding tension. The somatic component of EMDR can bypass these cognitive defenses if the therapist knows to watch for them. Understanding avoidant attachment patterns can help you recognize when you're doing this.
Disorganized attachment
AF-EMDR modifications are essential here—longer resourcing phases, careful titration of exposure, and constant monitoring of the window of tolerance. The reason: disorganized attachment can produce oscillation between flooding and dissociation during processing, with the nervous system alternating between "too much" and "nothing at all." Standard EMDR is most likely to destabilize clients with disorganized attachment because the protocol's pace doesn't account for this rapid switching. Both Wesselmann's family model and Parnell's AF-EMDR were designed with this population in mind.
Attachment-Style Processing Readiness Check (for all attachment styles)
- Identify your primary attachment style—anxious, avoidant, or disorganized
- Review the style-specific challenge in the section above
- Ask yourself: "When I think about processing a difficult relational memory, do I tend to flood with emotion, go blank or intellectual, or alternate between both?"
- Notice your answer without judgment—this is your nervous system's protective strategy, not a flaw
- Share this self-knowledge with any therapist you're considering working with—it helps them tailor the EMDR approach to your specific needs
This awareness is itself a form of earned security. You're developing the reflective functioning that securely attached people use naturally—the ability to observe your own patterns with curiosity rather than reactivity.
How does EMDR compare to other therapies for attachment?
EMDR targets memory reprocessing through the body, IFS works with internal protective parts, and EFT restructures attachment bonds within relationships—each addresses a different layer of the attachment system. There is no single best modality for attachment healing, and the right approach depends on your attachment style, your readiness, and whether you're working individually or with a partner.
| Feature | EMDR / AF-EMDR | IFS | EFT |
|---|---|---|---|
| Primary mechanism | Memory reprocessing via bilateral stimulation | Parts work and Self-energy | Restructuring attachment bonds in relationship |
| Processing direction | Bottom-up (body to cognition) | Inside-out (parts to Self) | Relational (partner to partner) |
| Best suited for | All styles; AF-EMDR especially for disorganized | All styles; especially disorganized (parts fragmentation) | Anxious-avoidant couples dynamics |
| Format | Individual | Individual | Couples or individual |
| Evidence for attachment change | Preliminary (pilot studies, N=3 to 20) | Emerging (case studies, mechanism-based) | Strong (20+ RCTs for couples) |
| Targets pre-verbal memory? | Yes (bilateral stimulation accesses implicit memory) | Yes (through somatic parts work) | Indirectly (through relational enactment) |
| Typical duration | 10 to 15 sessions for attachment | Open-ended, often 6 to 12+ months | 8 to 20 sessions (structured protocol) |
| Combines with others? | Yes—EMDR+IFS and EMDR+EFT both documented | Yes—IFS+EMDR increasingly common | Yes—EFT+EMDR for couples |
Integrative approaches are gaining traction. EMDR combined with IFS uses parts work to identify protectors before EMDR reprocessing—the IFS framework provides the map, EMDR provides the reprocessing engine. EMDR combined with EFT works well for couples: EMDR processes individual attachment wounds in separate sessions, then EFT restructures the couple's interaction patterns. Research on EMDR and EFT integration shows strong theoretical and clinical complementarity. For couples caught in the anxious-avoidant trap, this combination addresses both individual nervous system patterns and the relational cycle simultaneously.
Can EMDR make attachment issues worse?
Your concern about this is valid—and it reflects good self-protective instincts. The honest answer is yes, EMDR can destabilize when it's applied without proper attunement to attachment complexity. Knowing the retraumatization risk helps you protect yourself while remaining open to a therapy that may genuinely help.
Three scenarios increase the risk. Using the standard protocol with attachment-wounded clients who haven't had adequate resourcing is the most common problem. A therapist without attachment-specific training may miss signs that a client is dissociating during processing rather than integrating. And pushing processing when a client is outside their window of tolerance can reinforce the implicit belief that closeness leads to overwhelm—exactly what attachment therapy should be undoing.
Signs that EMDR isn't going well include increased dissociation between sessions, destabilized relationships, emotional flooding that doesn't resolve within a day or two of the session, and feeling more fragmented rather than more integrated over time.
The solution isn't avoiding EMDR—it's finding the right kind. AF-EMDR, with its emphasis on resourcing before processing, was designed specifically to address these risks.
Therapist Readiness Questions (for all attachment styles, especially disorganized)
Before starting EMDR, ask your potential therapist these questions: Are you trained in attachment-focused or modified EMDR protocols—not just the standard eight-phase model? How do you assess whether I'm ready for trauma processing versus needing more resourcing and stabilization? What is your approach if I dissociate during a session? How do you work with pre-verbal or implicit memories that don't have a clear visual image? What's your experience with complex or developmental trauma compared to single-incident trauma?
A therapist who can answer these questions thoughtfully has the training to work safely with attachment wounds. A therapist who seems confused by them or dismisses them may be excellent at standard EMDR but not the right fit for attachment-specific work. You deserve both competence and attunement.
When should you seek professional help?
EMDR is not a self-help technique—it requires a trained therapist to guide processing safely. The bilateral tapping exercises in this article offer a taste of the somatic component, but actual EMDR processing should never be attempted alone, especially for attachment-related material.
Consider EMDR or AF-EMDR if you've identified specific memories or patterns connected to your attachment style that talk therapy alone hasn't shifted. Your body holds relational trauma in ways that cognitive understanding can't always reach—persistent tension, numbness, exaggerated startle responses, or a nervous system that won't settle even when your mind knows you're safe.
Look for therapists with EMDRIA certification who also have specific training in developmental trauma or attachment-focused approaches. Standard EMDR certification alone doesn't guarantee expertise with relational wounds. Ask the therapist readiness questions above. Trust your nervous system's response in the first session—if you feel unsafe, that information matters.
The Meadow app can serve as a complement for between-session regulation—helping you build the daily nervous system awareness that makes EMDR sessions more productive. Healing your nervous system is both what happens in the therapy room and what you practice between sessions.
Frequently Asked Questions
What is attachment-focused EMDR?
Attachment-focused EMDR is Laurel Parnell's modification of standard EMDR designed for relational and developmental trauma. AF-EMDR adds resource tapping, emphasizes the therapeutic relationship as a corrective attachment experience, and uses a modified protocol that doesn't require a Positive Cognition—making it safer for clients with insecure attachment.
Can EMDR change your attachment style?
Preliminary research suggests EMDR can shift attachment classifications. Civilotti et al. (2019) found significant movement from insecure to secure attachment in 20 adults, and Barazzone et al. (2023) measured reduced fearful and dismissive attachment scores. No large-scale randomized trial exists yet, so evidence remains promising but not conclusive.
How many EMDR sessions are needed for attachment trauma?
Research suggests 10 to 15 sessions for attachment-related work, compared to 6 to 8 for single-incident PTSD. Disorganized attachment typically requires the longest course because more resourcing and stabilization time is needed before processing begins. AF-EMDR protocols often span several months.
What's the difference between EMDR and IFS for attachment trauma?
EMDR reprocesses traumatic memories through bilateral stimulation—a bottom-up, body-first approach. IFS works with internal protective parts and exiled emotions—an inside-out approach. EMDR changes how memories are stored, while IFS changes how you relate to your internal system. Many therapists now integrate both.
Can EMDR make attachment issues worse?
EMDR can destabilize when standard protocols are used without adequate resourcing for clients with complex attachment trauma. Risks include emotional flooding, increased dissociation, and destabilized relationships. Attachment-focused EMDR reduces these risks by building internal resources before processing. Choosing a therapist trained in developmental trauma is essential.
Does EMDR work for complex PTSD?
EMDR is recommended by WHO and APA for PTSD and shows growing evidence for complex PTSD, which frequently overlaps with attachment trauma. Modified protocols like attachment-focused EMDR and EMDR with extended stabilization phases are typically used for complex presentations rather than the standard eight-phase protocol.
What happens in the brain during EMDR?
Brain imaging studies show EMDR decreases amygdala activation, increases prefrontal cortex activity for stronger emotional regulation, and rebalances brain networks disrupted by trauma. Bilateral stimulation appears to mimic REM sleep processing, allowing traumatic memories to be reconsolidated with less emotional charge.
Is EMDR or talk therapy better for attachment?
EMDR may access pre-verbal and implicit memories that talk therapy cannot reach, since attachment patterns form before language develops. However, the therapeutic relationship in talk therapy is itself a corrective attachment experience. AF-EMDR combines both—the relational bond plus bilateral reprocessing—making it particularly suited for attachment work.
Want to Go Deeper?
Meadow includes a structured assessment to help you understand your specific attachment patterns, followed by a 66-day program of daily practices designed to build earned security.
Start your free week →References
Attachment and EMDR Research
Civilotti, C., Cussino, M., Callerame, C., Fernandez, I., & Gallina, L. (2019). Changing the adult state of mind with respect to attachment: An exploratory study on the use of EMDR in psychotherapy. Journal of EMDR Practice and Research, 13(3), 233–245.
Wesselmann, D., & Potter, A. E. (2009). Change in adult attachment status following treatment with EMDR: Three case studies. Journal of EMDR Practice and Research, 3(3), 178–191.
Barazzone, N., Katsimigos, A., Harrington-Morgan, H., & Nkrumah, I. (2023). EMDR and attachment security: A pilot study examining changes in attachment and symptoms over time. Journal of EMDR Practice and Research, 17(1), 38–52.
Wesselmann, D., Davidson, M., Armstrong, S., Schweitzer, C., Bruckner, D., & Potter, A. E. (2012). EMDR as a treatment for improving attachment status in adults and children. European Review of Applied Psychology, 62(4), 223–230.
General EMDR Evidence
American Psychological Association. (2017). Clinical practice guideline for the treatment of PTSD: EMDR. American Psychological Association.
EMDRIA. (2024). Recent research about EMDR therapy. EMDR International Association.
World Health Organization. (2013). Guidelines for the management of conditions specifically related to stress. WHO.
2024 meta-analysis on EMDR for depression: Hedges' g = 0.75 across 25 studies, N = 1,042. PMC.
Attachment-Focused EMDR
Parnell, L. (2008). Tapping in: A step-by-step guide to activating your healing resources through bilateral stimulation. Sounds True.
Parnell Institute. (2024). Clarifying the difference between EMDR and AF-EMDR. Parnell Institute.
Wesselmann, D., Schweitzer, C., & Armstrong, S. (2018). EMDR integrative group treatment protocol adapted for children with attachment trauma. Journal of EMDR Practice and Research, 12(4), 196–213.
Neuroscience
Amano, T., & Toichi, M. (2016). The role of alternating bilateral stimulation in establishing positive cognition in EMDR therapy: A multi-channel near-infrared spectroscopy study. PLOS ONE, 11(10), e0162735.
Boukezzi, S., El Khoury-Malhame, M., Auzias, G., Reynaud, E., Rousseau, P. F., Richard, E., ... & Khalfa, S. (2017). Grey matter density changes of structures involved in PTSD after recovery following EMDR therapy. Psychiatry Research: Neuroimaging, 266, 146–152.
Landin-Romero, R., Moreno-Alcazar, A., Pagani, M., & Amann, B. L. (2018). How does eye movement desensitization and reprocessing therapy work? A systematic review on suggested mechanisms of action. Frontiers in Psychology, 9, 1395.
EMDRIA. (2023). Keeping up with EMDR: The brain and neurobiology—from brain parts to brain networks. EMDR International Association.
Integrative Approaches
Halpern, S. C., Villanueva, A. O., Maieritsch, K. P., & Rosenberg, J. M. (2022). Combining EMDR and EFT in the treatment of couples: A conceptual integration. Journal of Marital and Family Therapy, 48(4), 1071–1087.
Sage Leaf Wellness. (2024). IFS and EMDR: A powerful combination for healing trauma. Sage Leaf Wellness.
This article is for educational purposes only and is not a substitute for professional mental health care. EMDR should only be performed by a trained, licensed therapist. If you are experiencing distress related to attachment trauma, please consult a qualified mental health professional.
