
Disorganized attachment is significantly linked to borderline personality disorder. Between 50 and 89 percent of individuals diagnosed with BPD display unresolved or disorganized attachment on the Adult Attachment Interview (Agrawal et al., 2004). Approximately 92 percent of people with BPD show insecure attachment overall, with disorganized attachment as the most characteristic pattern.
If you recognize disorganized attachment patterns in yourself and have wondered whether that means you "have BPD," you are not alone in that fear. The overlap between these two experiences is real—and confusing. But linked does not mean identical. This article breaks down what disorganized attachment and BPD share, where they diverge, and what you can actually do with that knowledge. Understanding the connection gives you clarity, not a diagnosis.
Key takeaway: Disorganized attachment is significantly linked to BPD, with 50 to 89 percent of people diagnosed with BPD showing disorganized attachment patterns. However, the two are distinct. Disorganized attachment is a risk factor that interacts with genetics, trauma severity, and mentalizing capacity. Many people with disorganized attachment never develop BPD, and attachment-focused healing can reduce BPD-related difficulties.
What do disorganized attachment and BPD actually share?
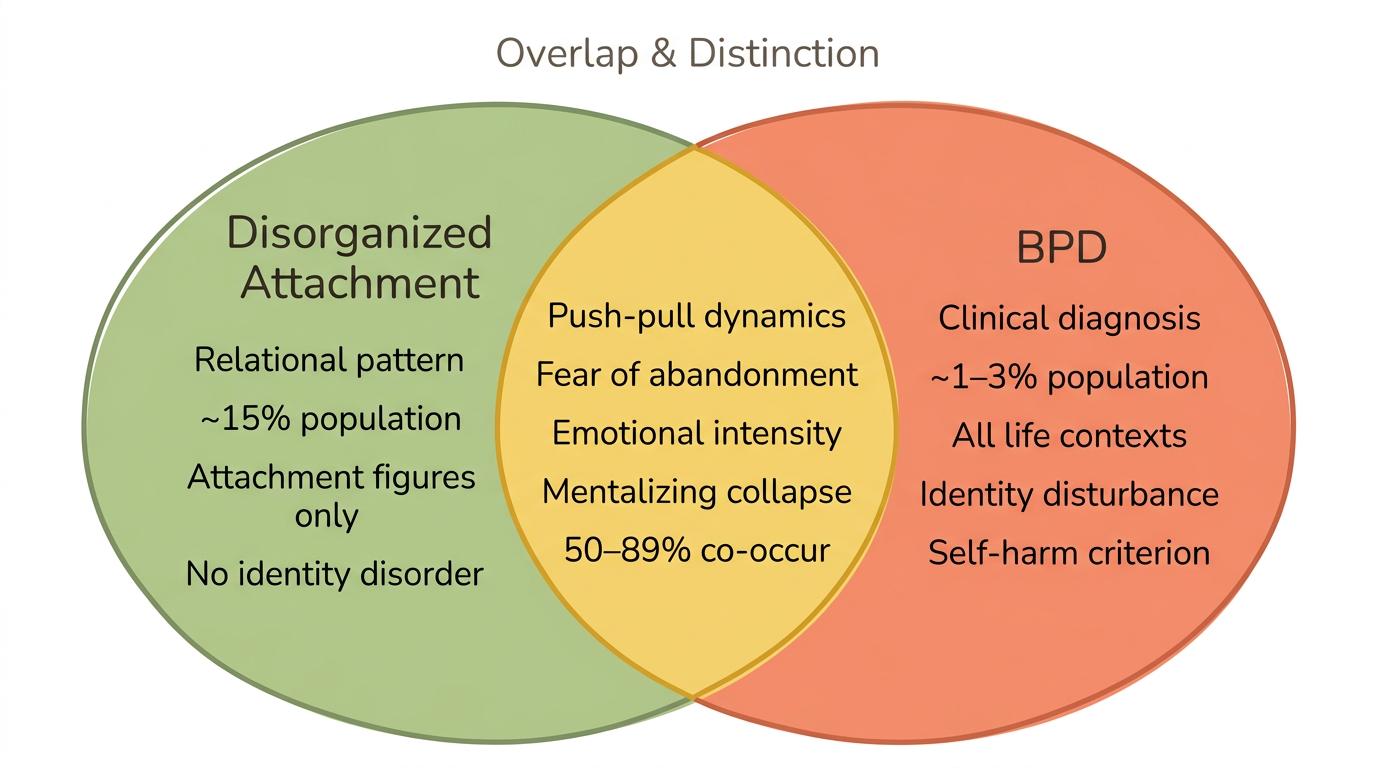
Disorganized attachment and BPD share a core experience: contradictory internal working models that create simultaneous, opposing impulses toward the people you need most. Both involve wanting closeness while fearing it, cycling between approach and withdrawal, and struggling to maintain a stable sense of self in relationships.
This overlap is well-documented. A meta-analysis by Scott et al. (2020) found that attachment anxiety correlates with BPD traits at r = 0.48, and attachment avoidance at r = 0.30—with the interaction of both (the hallmark of disorganized attachment) showing a "particularly strong relationship" to BPD pathology. 92 percent of people with BPD show insecure attachment, and the unresolved/disorganized classification appears far more frequently in BPD populations than in the general population (Agrawal et al., 2004).
The confusion between these two experiences makes sense. Both involve "fear without resolution"—your nervous system detects threat in the very person it seeks safety from. This produces the push-pull dynamics, emotional intensity, and dissociative moments that show up in both disorganized attachment and BPD. As Levy (2005) described, these represent "partially but not fully overlapping liabilities."
What this means in daily life: you might swing between desperately wanting reassurance and shutting down completely. You might feel like a different person depending on who you are with. Your body might toggle between hyperactivation—racing heart, urgent need to reach out—and collapse, where you feel numb or foggy. These are experiences shared across both disorganized attachment and BPD, rooted in the same early relational disruptions. The fawn response often emerges at this intersection—an attempt to manage the impossible tension between needing closeness and expecting harm.
The Both-And Check-In (for disorganized attachment)
- Recall a recent relational moment that felt confusing—where you wanted two opposite things at once
- Write "Part of me wanted..." and complete the sentence
- Below it, write "Another part of me wanted..." and complete that sentence too
- Notice which part felt more familiar or dominant
- Practice sitting with both without choosing—just noticing
This works for disorganized attachment because it externalizes the hostile-helpless oscillation that keeps you trapped between contradictory impulses. By naming both poles, you begin observing the pattern rather than being consumed by it.
How is disorganized attachment different from BPD?
If you have been trying to figure out whether your experience is "just" attachment or something more clinical, that uncertainty itself is worth honoring. Disorganized attachment is a risk factor, not a diagnosis. It describes a relational pattern formed in infancy when a caregiver was simultaneously the source of comfort and the source of fear. BPD is a clinical disorder defined by the DSM-5, involving multiple domains of functioning beyond attachment relationships alone.
Not everyone with disorganized attachment develops BPD. Research by Levy (2005) found that "only a subgroup of insecurely attached individuals develops BPD," suggesting that additional factors mediate the pathway. Lenzenweger and Cicchetti (2018) found that being disorganized with both parents—not just one—was particularly characteristic of adolescents with BPD, and this predicted group membership over and above reported trauma history.
The multi-pathway model helps explain why. BPD develops through an interaction of genetic vulnerability, the severity and chronicity of early trauma, the availability of other supportive relationships, and the development of mentalizing capacity (Fonagy and Bateman, 2008). Disorganized attachment is one ingredient—a significant one—but not the only one.
Here are five key differences:
- Scope: Disorganized attachment is a relational pattern activated primarily with attachment figures. BPD is a clinical disorder that affects identity, impulse control, self-image, and emotional regulation across many contexts.
- Context-dependence: You might function well at work and with friends while experiencing intense disorganized patterns only in intimate relationships. BPD features tend to show up more broadly.
- Severity threshold: Disorganized attachment exists on a spectrum. BPD requires meeting a specific threshold of diagnostic criteria.
- Identity disturbance: Disorganized attachment involves contradictory implicit relational models—you expect both care and harm. BPD involves a more pervasive, chronic sense of not knowing who you are.
- Self-harm and impulsivity: These are not defining features of disorganized attachment. They are central diagnostic criteria for BPD.
Disorganized attachment vs. BPD: what's shared and what's distinct
| Feature | Disorganized Attachment | BPD |
|---|---|---|
| Origin | Infant-caregiver relationship pattern | Clinical diagnosis (DSM-5) requiring multiple criteria |
| Fear of abandonment | Present in close relationships | Pervasive, frantic efforts to avoid real or imagined abandonment |
| Relationship instability | Approach-avoid cycling with attachment figures | Intense, unstable relationships across contexts |
| Identity | Contradictory internal working models | Chronic identity disturbance and emptiness |
| Emotional dysregulation | Activated by attachment threats | Persistent across many contexts |
| Dissociation | May occur under attachment stress | Transient, stress-related paranoia or dissociation |
| Self-harm / impulsivity | Not a defining feature | Central diagnostic criterion |
| Mentalizing breakdown | Under attachment-specific stress | Broader, more pervasive |
| Prevalence | Approximately 15 percent of general population | 0.6–3 percent of general population |
| Can it change? | Yes—earned security through relationship and therapy | Yes—highly treatable with evidence-based therapy |
For more on how disorganized and fearful-avoidant attachment relate to each other, that distinction adds another helpful layer of clarity.
What role does mentalization play in the attachment-BPD connection?
Mentalization—the ability to understand your own and others' minds—is the bridge that connects disorganized attachment to BPD vulnerability. When your attachment system detects threat, your capacity to mentalize shuts down. You stop being able to hold your own mental states and others' mental states in mind simultaneously (Fonagy and Bateman, 2008).
This matters because attachment hyperactivation suppresses mentalizing. When you feel abandoned, rejected, or threatened by someone you love, your nervous system floods with alarm signals. In that state, your brain cannot do the nuanced work of considering multiple perspectives. Instead, you fall into what Fonagy calls "pre-mentalizing modes"—more primitive ways of making sense of what is happening.
These pre-mentalizing modes look like this in everyday life:
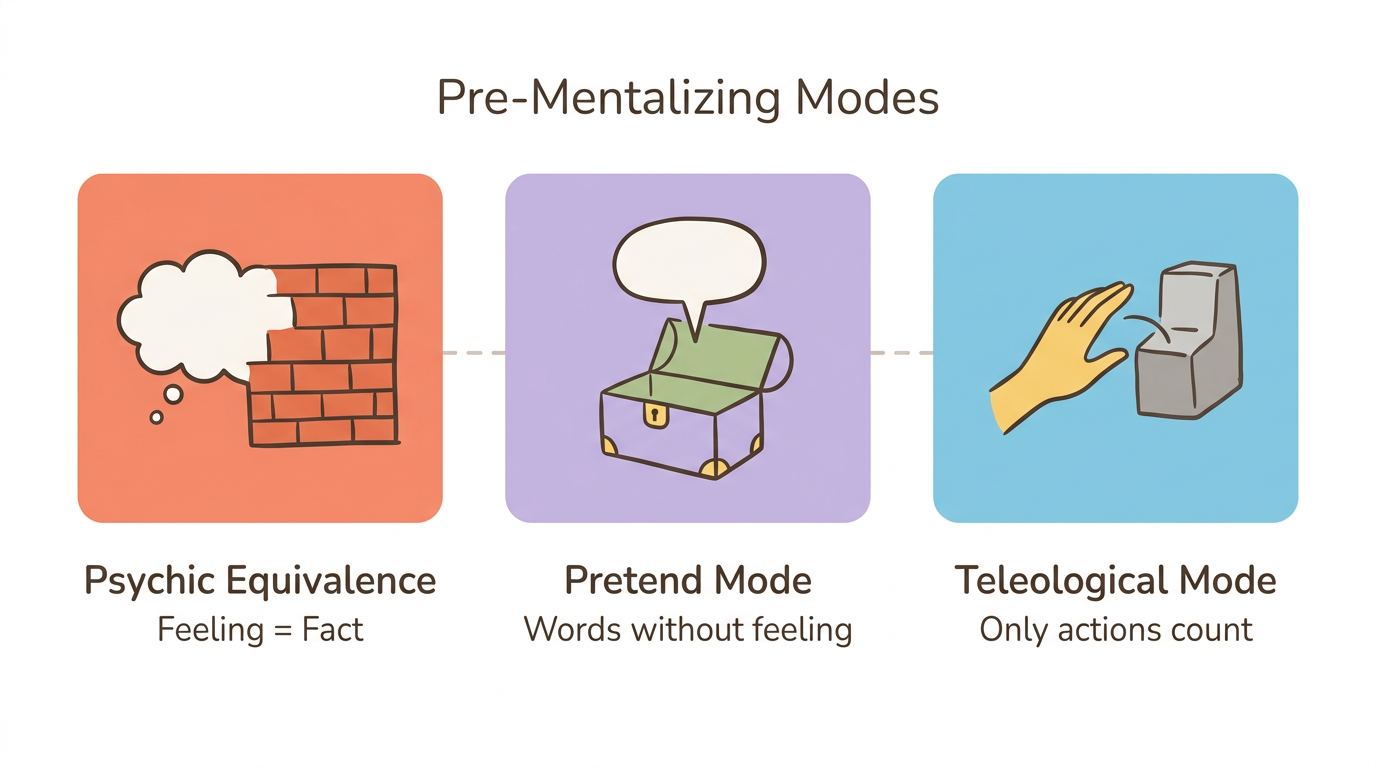
- Psychic equivalence: "I feel rejected, therefore I am being rejected." Your internal experience feels like an absolute fact about external reality. There is no gap between feeling and knowing.
- Pretend mode: Imagine sitting in therapy, speaking fluently about your childhood, sounding deeply insightful—while feeling absolutely nothing in your body. The words are real but disconnected from your actual emotional experience.
- Teleological mode: Your partner says "I love you," but your nervous system does not register it. Only concrete, visible actions count—a text back within minutes, physical presence, a specific gesture. Abstract reassurance cannot land when your system is in this mode.
When a child grows up with a caregiver who is frightening or frightened, their developing mentalizing capacity never gets the stable foundation it needs. The very person who should help the child make sense of their internal world is the source of confusion. This is why disorganized attachment is so hard to heal—the system designed for understanding minds developed under conditions that made understanding minds dangerous.
Mentalization-based treatment (MBT), developed specifically for BPD by Fonagy and Bateman, targets exactly this breakdown. A systematic review found MBT produces effect sizes of d = 0.59 to 1.79 for BPD symptom reduction, with an 8-year follow-up showing continued improvement five or more years post-treatment (Bateman and Fonagy, 2008).
The Mentalizing Pause (somatic technique for disorganized attachment)
- Notice a moment of relational intensity—racing heart, tunnel vision, absolute certainty about what someone else is thinking
- Place one hand on your chest and feel the contact
- Take three slow breaths, making the exhale longer than the inhale
- Ask yourself: "Am I guessing or do I actually know what they are feeling right now?"
- Name one alternative explanation for their behavior—even if you do not fully believe it yet
This interrupts the collapse of mentalizing that drives hostile-helpless oscillation in disorganized attachment. The somatic grounding—hand on chest, slow exhale—activates the ventral vagal pathway to widen your window of tolerance before you re-engage relationally.
What does the neuroscience tell us about the overlap?
Neuroscience confirms that disorganized attachment and BPD share overlapping changes in brain structure and stress response systems, shaped by early relational trauma. These are not abstract psychological concepts—they have biological signatures that neuroscience can observe.
The amygdala: your threat detection system
Individuals with disorganized attachment show larger amygdala volumes in adulthood, with larger left amygdala volume strongly related to dissociative symptoms (Arancibia et al., 2023). BPD similarly involves amygdala hyperactivation in response to attachment-related stimuli. Your threat detection system adapted to match the level of vigilance your early environment required.
The stress response: cortisol and the HPA axis
Disorganized infants show a flattened diurnal cortisol rhythm compared to non-disorganized children—their stress response system loses its natural rise-and-fall pattern (Arancibia et al., 2023). BPD is associated with HPA axis hyperactivation and heightened stress sensitivity. When your stress system was calibrated by unpredictable caregiving, it adapted by staying perpetually on alert or shutting down entirely.
Prefrontal regulation: the braking system
Adults with disorganized attachment show greater activation of the anterior cingulate cortex when processing attachment-related threats (Arancibia et al., 2023). BPD shows reduced prefrontal regulation of amygdala responses—meaning the brain's braking system struggles to slow down the alarm signals. Your body is not overreacting. It is responding proportionally to what it learned to expect.
The shared neural substrate tells us something hopeful: both disorganized attachment and BPD involve disrupted development of brain structures during critical periods, but neuroplasticity means these patterns can change. Your brain adapted to early danger—and it can adapt again to new experiences of safety.
Stress Signature Mapping (body-based technique for disorganized attachment)
- On a piece of paper, draw a simple body outline
- During a calm moment, recall a recent situation where an attachment figure triggered you
- Mark where you felt activation—tight chest, clenched jaw, numb limbs, foggy head, stomach drop
- Next to each mark, note whether it felt like hyperactivation (fight, flight, urgency) or hypoactivation (freeze, numbness, dissociation)
- This is your stress signature—the unique map of how your nervous system oscillates between alarm and shutdown
This builds interoceptive awareness of the oscillation between hyperactivation and dissociation that characterizes the disorganized nervous system. Share your map with your therapist or use it as an early warning system—noticing the first sensations before the full cascade arrives.
Can healing disorganized attachment reduce BPD symptoms?
Yes—and research strongly supports this. If disorganized attachment is a pathway into BPD features, then attachment healing is a pathway out. Your nervous system learned these patterns in relationship, and relationship—including the therapeutic relationship—is where they can shift.
Your body developed these responses for good reason. The hypervigilance, the oscillation between reaching out and shutting down, the difficulty trusting your own perceptions—all of these made sense in the context where they formed. And now, with support, you can teach your nervous system something new.
Several evidence-based approaches directly target the attachment-BPD connection:
-
Mentalization-Based Treatment (MBT) most directly addresses the mentalizing breakdown that links disorganized attachment to BPD. Patients show continued improvement five or more years post-treatment, with effect sizes of d = 0.59 to 1.79 (Bateman and Fonagy, 2008).
-
The most empirically supported BPD treatment overall, Dialectical Behavior Therapy (DBT) targets emotion dysregulation, distress tolerance, and interpersonal effectiveness. It does not explicitly target attachment but addresses the downstream symptoms that cause the most daily suffering.
-
Transference-Focused Psychotherapy (TFP) works with attachment patterns as they emerge live in the therapeutic relationship—the split internal working models, the part that idealizes and the part that devalues, become visible and workable in real time.
-
Many people find that Schema Therapy names what they have always felt: early maladaptive schemas like abandonment, mistrust, and emotional deprivation that map onto insecure attachment patterns. Evidence supports BPD symptom remission.
-
For those who experience the contradictory internal models of disorganized attachment as distinct "parts," Internal Family Systems (IFS) offers a framework to meet the hostile part and the helpless part with curiosity rather than being blended with either one.
-
When specific attachment trauma memories drive disorganized patterns, EMDR can reduce their emotional charge so your nervous system no longer responds to present-day relationships as if past danger were still happening.
For a deeper look at which therapies work best for disorganized attachment and realistic expectations around how long healing takes, those guides provide more detailed roadmaps.
You don't rewire attachment in a single insight. You rewire it by noticing 10 percent earlier, responding 10 percent differently, 10 percent more often.
Parts Dialogue (IFS-informed, for disorganized attachment)
- Identify a recent moment where you felt "split"—part of you hostile, angry, or pushing away, and part of you helpless, collapsed, or desperate for closeness
- Give each part a name or an image—whatever comes naturally
- Write a brief dialogue. Ask the hostile part: "What are you trying to protect me from?" Ask the helpless part: "What do you need right now?"
- Notice: can you hold both with curiosity rather than being consumed by either one?
- Write one sentence to each part, acknowledging what it does for you
This directly addresses the hostile-helpless oscillation that Lyons-Ruth et al. (2007) identified as characteristic of BPD-linked disorganized attachment. In their study, 100 percent of women with BPD displayed contradictory hostile-helpless states of mind, compared to 50 percent of women with dysthymia. By dialoguing with both parts, you practice the Self-energy that IFS cultivates—the capacity to witness your parts without being overtaken by them.
When should you seek professional support?
If you recognize yourself in both columns of the comparison table above, that recognition is a sign of self-awareness—not a diagnosis. Reading an article cannot replace a clinical assessment, and you deserve more than a self-administered label.
That said, certain experiences warrant reaching out to a mental health professional who understands both attachment and personality disorders. BPD is highly treatable, and early intervention makes a meaningful difference.
Here are five signs that professional assessment would be helpful:
- If you are hurting yourself or thinking about it, please reach out. Self-harm or suicidal thoughts go beyond attachment patterns and need clinical support—this is the most important reason not to wait.
- Chronic emptiness: A persistent feeling of hollowness or not knowing who you are—not just in relationships but across your life.
- Do you feel like a fundamentally different person depending on who you are with? Not the normal social flexibility everyone experiences, but a deeper identity instability that leaves you unsure which version of you is real.
- Losing time, feeling detached from your body, or experiencing the world as unreal—especially when triggered by relational stress—these dissociative episodes signal that your nervous system needs more support than self-help alone can provide.
- A pattern of relationship rupture without repair: Relationships that repeatedly end in explosive conflict or abrupt cutoff, without the capacity to work through disagreements.
Recognizing yourself in this article is a sign of strength, not a reason for shame. Whether what you are experiencing is disorganized attachment, BPD, both, or something else entirely, "quiet BPD"—internalized presentations where the turmoil stays hidden—is especially common among people who would seek out an article like this one. You do not need to meet a dramatic stereotype to deserve support.
Can disorganized attachment be healed? Yes—and professional support is the most reliable path to doing so.
Frequently Asked Questions
Is disorganized attachment the same as BPD?
No. Disorganized attachment is a relational pattern formed in early childhood when a caregiver was both a source of comfort and a source of fear. BPD is a clinical diagnosis involving identity disturbance, self-harm, and emotional dysregulation across many life contexts. Research shows 50 to 89 percent of people with BPD have disorganized attachment, but many with disorganized attachment never develop BPD.
What attachment style is most common in BPD?
Unresolved or disorganized and preoccupied attachment are the most characteristic patterns. Research shows 92 percent of people with BPD have insecure attachment, with 50 to 89 percent classified as unresolved or disorganized on the Adult Attachment Interview. Secure attachment appears in only zero to eight percent of BPD samples.
Can you have disorganized attachment without BPD?
Yes—most people with disorganized attachment do not develop BPD. Disorganized attachment affects roughly 15 percent of the general population, while BPD affects 0.6 to 3 percent (Agrawal et al., 2004). Genetic predisposition, trauma severity, and mentalizing capacity all influence whether disorganized attachment leads to BPD.
Can BPD be caused by attachment trauma?
Attachment trauma is a significant risk factor but not the sole cause. Longitudinal research shows that maternal withdrawal in infancy predicts borderline symptoms in adolescence. BPD develops through an interaction of genetic vulnerability, attachment disruption, and impaired mentalizing capacity (Fonagy and Bateman, 2008).
What is mentalization and how does it relate to BPD?
Mentalization is the ability to understand your own and others' thoughts, feelings, and motivations. When the attachment system is hyperactivated by perceived threat, mentalizing capacity shuts down—leading to misreading intentions and reactive behavior (Fonagy and Bateman, 2008). Mentalization-based treatment targets this mechanism and shows strong results for BPD.
Does healing attachment heal BPD?
Attachment-focused therapies show strong results for BPD symptoms. Mentalization-based treatment, developed specifically from attachment theory, produces effect sizes of d = 0.59 to 1.79 for BPD symptom reduction, with continued improvement five or more years post-treatment (Bateman and Fonagy, 2008). Healing attachment patterns addresses a core vulnerability underlying BPD.
What does BPD look like in relationships vs. disorganized attachment?
Both involve push-pull relationship dynamics and fear of abandonment. The difference is scope: disorganized attachment patterns primarily activate with close attachment figures, while BPD features—identity disturbance, chronic emptiness, impulsivity—extend across many life contexts beyond relationships. Levy (2005) described these as "partially but not fully overlapping liabilities."
Is BPD a trauma response or a personality disorder?
Current research supports both perspectives. BPD is classified as a personality disorder in the DSM-5, but its strong links to early attachment trauma have led many clinicians to view it as a complex trauma response. These frameworks are not mutually exclusive.
Want to Go Deeper?
Meadow includes a structured assessment to help you understand your specific attachment patterns, followed by a 66-day program of daily practices designed to build earned security.
Start your free week →References
Attachment and BPD Reviews
-
Agrawal, H. R., Gunderson, J., Holmes, B. M., & Lyons-Ruth, K. (2004). Attachment studies with borderline patients: A review. Attachment & Human Development, 6(3), 241–263.
-
Levy, K. N. (2005). The implications of attachment theory and research for understanding borderline personality disorder. Attachment & Human Development, 7(3), 299–312.
-
Scott, L. N., Kim, Y., Nolf, K. A., Hallquist, M. N., Wright, A. G. C., Stepp, S. D., Morse, J. Q., & Pilkonis, P. A. (2020). Preoccupied attachment and emotional dysregulation: Specific aspects of borderline personality disorder or general dimensions of personality pathology? Clinical Psychology Review, 76, 101837.
Empirical Studies
-
Lenzenweger, M. F., & Cicchetti, D. (2018). Toward a developmental psychopathology approach to borderline personality disorder. Frontiers in Psychology, 9, 1962.
-
Lyons-Ruth, K., Melnick, S., Patrick, M., & Hobson, R. P. (2007). A controlled study of hostile-helpless states of mind among borderline and dysthymic women. Attachment & Human Development, 9(1), 1–16.
-
Lyons-Ruth, K. (2008). Contributions of the mother-infant relationship to dissociative, borderline, and conduct symptoms in young adulthood. Infant Mental Health Journal, 29(3), 203–218.
Mentalizing and Treatment
-
Fonagy, P., & Bateman, A. W. (2008). The development of borderline personality disorder—A mentalizing model. Journal of Personality Disorders, 22(1), 4–21.
-
Bateman, A., & Fonagy, P. (2008). 8-year follow-up of patients treated for borderline personality disorder: Mentalization-based treatment versus treatment as usual. American Journal of Psychiatry, 165(5), 631–638.
-
Effectiveness of mentalization-based treatment for borderline personality disorder: A systematic review. (2019). PMC, PMC6900007.
Neuroscience
- Arancibia, M., Varela, J., Cerda, J., & Sánchez, C. (2023). Neurobiology of disorganized attachment: A review. Neuroscience Insights, 18.
Clinical Context
-
Psychology Today. (2021). Attachment styles and borderline personality disorder.
-
The Attachment Project. (n.d.). BPD and attachment style.
This article is for educational purposes only and is not a substitute for professional mental health assessment or treatment. If you are experiencing thoughts of self-harm or suicide, please contact the 988 Suicide and Crisis Lifeline by calling or texting 988, or reach out to a mental health professional in your area. Disorganized attachment and BPD are both highly responsive to evidence-based treatment—reaching out for support is an act of courage.
