
Avoidant attachment is a relational pattern where emotional closeness triggers withdrawal rather than comfort. If closeness has always felt more threatening than comforting, that pattern makes sense. Approximately 22 to 25 percent of adults have avoidant attachment (Mickelson et al., 1997). The core answer is yes—avoidant attachment can be healed. Research on earned secure attachment demonstrates that people who were insecurely attached in childhood can develop security in adulthood through reflection, corrective relationships, and targeted therapeutic work (Roisman et al., 2002).
Healing avoidant attachment requires moving toward the very thing your nervous system has learned to treat as threatening—emotional closeness. That protective distance you keep isn't a character flaw. Your nervous system developed this pattern because, at some point, it was the safest option available to you. If you're still unsure whether this applies to you, start with identifying avoidant patterns. This article is a science-backed guide to understanding why avoidant patterns persist and what actually shifts them.
Key takeaway: Yes, avoidant attachment can be healed through a process called earned secure attachment. Research shows approximately 30 percent of people shift attachment styles over time, and therapies like Emotionally Focused Therapy and somatic approaches produce measurable reductions in avoidance. Healing requires recognizing deactivating strategies, reconnecting with suppressed emotional needs, and building tolerance for closeness through graduated practice.
What Does It Mean to "Heal" Avoidant Attachment?
Healing avoidant attachment means developing what researchers call earned secure attachment—not erasing avoidant tendencies but building the capacity to recognize them and choose differently. Mary Main first introduced this concept through the Adult Attachment Interview, showing that individuals who develop coherent narratives about difficult childhood experiences can shift from insecure to secure classification.
A 23-year longitudinal study tracked infants to age 22 and documented this trajectory from insecure to earned-secure attachment (Roisman et al., 2002). The mechanism was not forgetting the past but developing reflective functioning—the ability to make sense of early experiences without minimizing or being overwhelmed by them. Research confirms that attachment styles can and do change, with Kirkpatrick and Hazan finding that 30 percent of people change attachment style over a four-year period.
Healing doesn't look like becoming a different person. You may always notice the pull toward independence when stress rises. The difference is that pull no longer runs the show. You notice it, breathe through it, and make a conscious choice about how to respond.
Your nervous system learned to equate closeness with threat for good reason—it kept you safe. And now, through earned security, you can teach it that closeness can also mean safety.
The Coherent Narrative Check-In (for dismissive-avoidant attachment)
- Write 3 to 4 sentences about a childhood moment when you needed comfort but didn't receive it
- Read what you wrote and notice your internal response
- Are you minimizing ("it wasn't a big deal")? Intellectualizing ("it made me resilient")? Feeling disconnected from the memory entirely?
- Name what you notice without trying to change it: "I notice I'm minimizing this"
- Sit with that noticing for 30 seconds
This builds reflective functioning—the core mechanism of earned security. Dismissive-avoidant individuals often intellectualize childhood experiences, and this exercise interrupts that pattern by making the intellectualization itself visible.
For a deeper understanding of earned security, see what earned secure attachment means.
Why Does Avoidant Attachment Feel So Hard to Change?
Avoidant attachment resists change because the brain and body actively work to maintain emotional distance—even when the conscious mind wants connection. Three neuroscience mechanisms explain why healing feels so counterintuitive.
First, connection doesn't register as rewarding in the avoidant brain. fMRI research shows avoidant individuals have decreased activation in the anterior insula and dorsal anterior cingulate cortex during social exclusion—areas that typically signal social pain (DeWall et al., 2012). Reduced activation in reward circuits when viewing scenes of comfort means that closeness literally produces less neurological reward than it does for securely attached individuals. Attachment avoidance also correlates with reduced gray matter density in the hippocampus (BMC Neuroscience, 2021).
Second, avoidant individuals can't accurately read their own stress. Research reveals a dissociation between psychological and endocrine stress measures—avoidant individuals report low distress but show elevated cortisol. Your body is sounding the alarm while your mind insists everything is fine.
Third, Mikulincer and Shaver's research on deactivating strategies shows that avoidant individuals block conscious access to attachment needs—but not unconscious activation. Your need for connection exists—you just can't feel it. The attachment system fires below awareness while suppression strategies keep it from reaching consciousness.
Here are the four core deactivating strategies that maintain avoidant patterns:
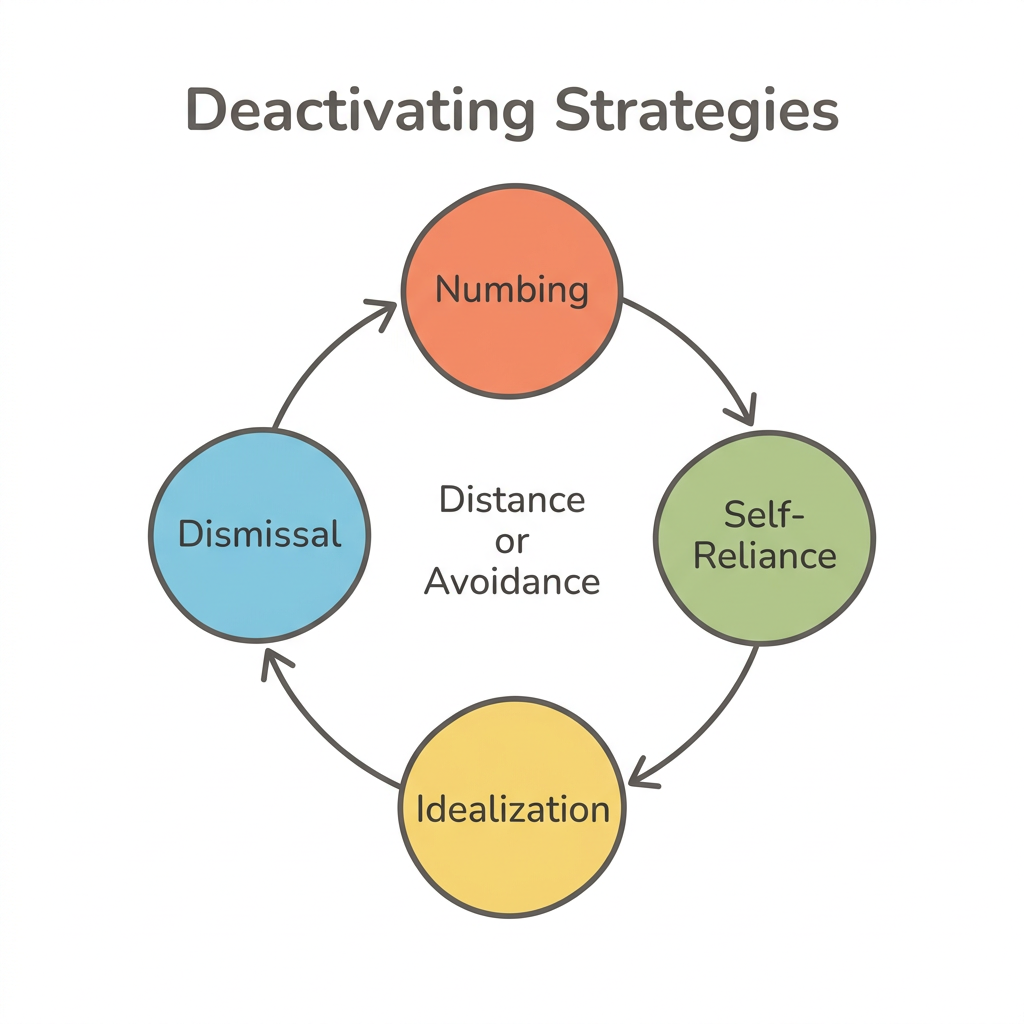
- Emotional numbing—flattening feelings when closeness increases, creating a sense of going blank during intimate conversations
- Compulsive self-reliance—refusing help even when struggling, treating any need as weakness
- Isolation becomes strength in the avoidant mind. Idealization of independence reframes protective distance as freedom, making the pattern feel chosen rather than compulsive
- When a partner expresses emotional needs, dismissal kicks in—their feelings get minimized, rationalized, or redirected to maintain comfortable distance
This push-pull pattern is common in fearful-avoidant attachment and can look different depending on whether the avoidant style is dismissive or fearful.
Your body adapted brilliantly to an environment where emotional closeness wasn't safe. That adaptation kept you functioning. And now it may be running a protection program that no longer matches your reality.
The Body Scan for Hidden Stress (somatic technique for avoidant attachment)
- Set a timer for 2 minutes
- Close your eyes and rate your current stress level from 1 to 10
- Slowly scan from the top of your head to your feet, pausing at each area for 5 seconds
- Notice areas of tension, numbness, or blankness—these are common in avoidant patterns because the nervous system suppresses distress signals
- When you find tension or numbness, breathe gently into that area without trying to fix it
- After the scan, rate your stress again from 1 to 10
Avoidant individuals often discover their body holds stress their mind dismissed. This exercise addresses the cortisol-psychology dissociation by building interoceptive awareness—the ability to read your own body's signals—which is often underdeveloped in avoidant attachment because the nervous system learned to mute those signals early.
What Therapy Works Best for Avoidant Attachment?
Standard talk therapy alone is often insufficient for avoidant attachment. The Levy and Johnson (2018) meta-analysis—spanning 36 studies and 3,158 participants—found that avoidance was uncorrelated with general therapy outcome, meaning avoidant individuals need specialized treatment that directly targets relational and emotional processing rather than generic approaches.
If you're reading this section and noticing reluctance—a pull to skip ahead or tell yourself you can figure this out alone—that's worth paying attention to. Researching therapy options can itself activate the avoidant system, and that resistance is information, not a verdict.
Here is what the evidence supports:
| Approach | Best For | Core Mechanism | Evidence Level | Key Benefit for Avoidant Individuals |
|---|---|---|---|---|
| EFT | Couples | Withdrawer re-engagement and softening | Strong (20+ outcome studies) | Directly targets pursue-withdraw cycle |
| CBT + Interpersonal/Emotional Processing | Both | Schema modification + emotional awareness | Strong (RCT) | Addresses cognitive and emotional avoidance together |
| ABCT | Both | Compassion cultivation for attachment | Moderate (RCT) | Builds self-compassion without requiring a partner |
| IFS | Both | Protector parts dialogue | Moderate (clinical) | Non-threatening: approaches avoidance as a "part," not a flaw |
| Somatic Experiencing | Both | Body-based trauma processing | Moderate (clinical) | Bypasses intellectualization; reaches stored body-level patterns |
| Self-directed practices | Both | Graduated exposure to vulnerability | Emerging | Accessible daily; builds on micro-dose research |
| DBT Skills | Both (especially fearful-avoidant) | Distress tolerance + emotion regulation | Moderate | On-ramp that doesn't require immediate emotional exposure |
Emotionally Focused Therapy
Emotionally Focused Therapy (EFT) carries the strongest evidence for avoidant patterns in couples, with a 70 to 75 percent recovery rate for distressed couples (Johnson, 2019). The core intervention for avoidant partners is withdrawer re-engagement—a structured process where the withdrawing partner learns to express attachment needs instead of shutting down. The softening event—when the avoidant partner allows vulnerability—produces significant increases in relationship satisfaction and reductions in attachment avoidance. If you're caught in the anxious-avoidant trap, EFT directly targets this cycle.
Individual Therapy Approaches
Newman et al. (2015) found that highly dismissing-avoidant patients showed significantly greater symptom change when CBT was augmented with interpersonal and emotional processing compared to CBT with supportive listening alone. Attachment-Based Compassion Therapy produced significant reductions in attachment avoidance and increases in secure attachment (Navarro-Gil et al., 2018). Even severe avoidant presentations can shift—a case documented in the American Journal of Psychotherapy (2016) showed remission of avoidant personality disorder through the therapeutic relationship.
Your resistance to therapy isn't a personal failing. It's your attachment system doing exactly what it was designed to do—keeping you at a safe distance. Recognizing that resistance as a data point rather than an obstacle is itself a therapeutic act.
The Withdrawer Re-Engagement Script (adapted from EFT, for dismissive-avoidant attachment)
- Notice the urge to withdraw—you might feel a tightening in your chest, a desire to change the subject, or mental fog
- Name the urge internally: "I'm wanting to shut down right now"
- Share one layer with your partner: "I'm noticing I want to pull away from this conversation"
- Add one feeling word: "I think I feel [overwhelmed / pressured / scared]"
- Make one request: "Can we slow down?" or "Can you give me a moment?"
This graduated disclosure builds the muscle of staying present without requiring full vulnerability. It works for dismissive-avoidant individuals because it interrupts the withdraw reflex at the earliest stage—when the urge first appears—rather than asking for deep emotional sharing, which activates the deactivating system. For more on expressing needs safely, see how to communicate without triggering your partner.
Can You Heal Avoidant Attachment Without Therapy?
Therapy accelerates healing significantly, but daily relationship practices also produce measurable shifts in avoidant attachment. Research shows that trust uniquely predicted reduced avoidance over time—meaning consistent, reliable relationship experiences can gradually rewire avoidant patterns even outside a therapist's office (Kirkpatrick and Hazan).
Chopik (2024) reviewed evidence showing that frequent daily positive relationship events predict reduced attachment avoidance—what might be called a micro-dose approach to earned security. Small moments of received care, shared vulnerability, and tolerated closeness accumulate into genuine pattern shifts. You don't rewire avoidant attachment in a single breakthrough. You rewire it by staying 10 percent longer in a conversation that makes you uncomfortable, 10 percent more often.
Dismissive-Avoidant vs. Fearful-Avoidant Healing Paths
Understanding the distinction between dismissive-avoidant and fearful-avoidant healing paths matters because the work looks different for each.
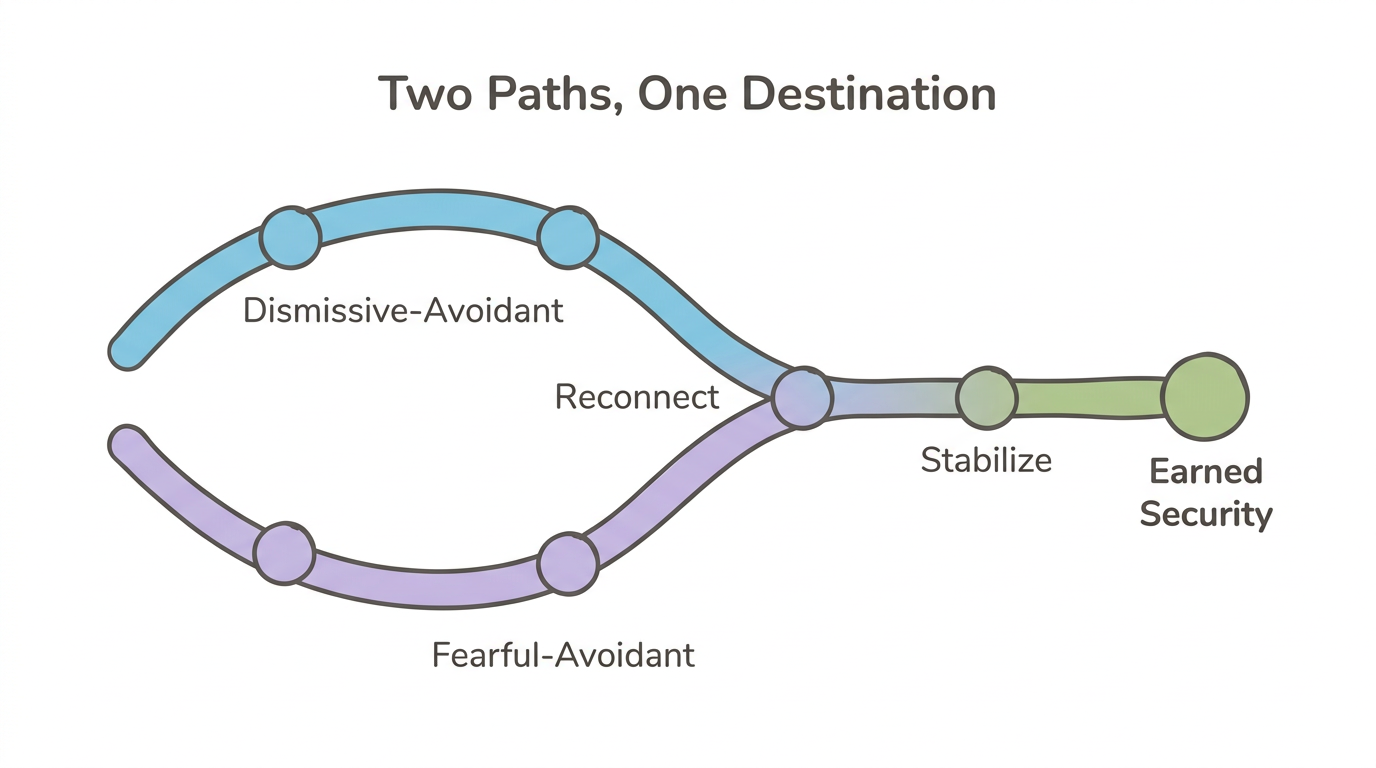
Dismissive-avoidant individuals need to reconnect with emotions they've learned to suppress. The primary challenge is accessing feelings at all—many describe emotional blankness or intellectualize when asked how they feel. Healing involves building interoceptive awareness and learning to identify and name emotional states.
Fearful-avoidant individuals need to build stability within emotional experiences. They already feel intensely but oscillate between craving closeness and pulling away. Healing involves learning to tolerate emotional activation without either merging with another person or fleeing from them.
Both paths lead toward the same destination—earned security—but through different terrain. For a full guide to building security, see how to develop secure attachment as an adult.
What you've done on your own already matters. Every moment you noticed the urge to pull away and chose to stay—even briefly—was your nervous system learning something new. That learning counts, even without a therapist in the room.
The 5-Minute Vulnerability Window (for avoidant individuals who find open-ended emotional conversations overwhelming)
- Choose one person you trust
- Set a timer for 5 minutes where they can see it
- Share one thing you're struggling with—not a problem to solve, but a feeling to express
- When the timer ends, you can stop. No obligation to continue
- Notice what happens in your body as you share—tightness, numbness, the urge to deflect with humor
- Practice weekly, gradually extending to 7, then 10 minutes
The bounded container makes emotional sharing feel safer for avoidant nervous systems by providing a clear exit point. This works with—not against—the deactivating system. Instead of asking you to "be more open" with no endpoint, it gives your nervous system a predictable boundary, which reduces the threat activation that typically triggers withdrawal.
How Does the Nervous System Change During Avoidant Healing?
The nervous system shifts from automatic shutdown to flexible engagement as avoidant attachment heals. Through the lens of polyvagal theory (Porges), avoidant attachment maps to dorsal vagal shutdown—the freeze or collapse response that activates when intimacy is invited. Your nervous system treats closeness the way another person's might treat physical danger: by shutting down, going numb, or mentally checking out.
Healing involves expanding your window of tolerance—the range of emotional and relational intensity you can stay present within before your nervous system hits the emergency brake. When that window is narrow, even a partner asking "how are you feeling?" can trigger dorsal vagal shutdown. As the window expands, that same question registers as an invitation rather than a threat.
Neuroplasticity provides the biological foundation for this shift. Avoidant individuals show lower oxytocin levels and reduced reward circuit activation for social bonding. But these neural patterns aren't fixed—secure relationships and therapeutic experiences can rewire attachment-related circuits through repeated corrective experiences. Your attachment style shapes how your nervous system responds to closeness, and that response can change.
The shift doesn't happen all at once. Healing looks like your dorsal vagal response firing a few seconds later than it used to. Then a few seconds later than that. Over months and years, what once felt unbearable—sitting with someone's emotional presence—becomes tolerable, then familiar, then even welcome.
The Deactivation Pause (somatic technique for avoidant activation in relational moments)
- When you feel the pull to withdraw—the mental fog, the urge to change the subject, the sudden need to be alone—physically stop for 30 seconds
- Place one hand on your chest
- Notice your breathing—avoidant deactivation often involves shallow breathing or breath-holding
- Take 3 slow breaths with a longer exhale than inhale (inhale for 4 counts, exhale for 6 counts)—the extended exhale activates the ventral vagal system, signaling safety
- After 30 seconds, choose: you can still withdraw, but you're choosing from awareness rather than autopilot
This pause works with the dorsal vagal shutdown pattern by introducing ventral vagal engagement at the moment deactivation begins. Over time, it expands your window of tolerance for closeness—not by forcing you to stay, but by giving your nervous system a moment to recalibrate before the protective shutdown completes.
When Should You Seek Professional Help for Avoidant Attachment?
Professional support becomes important when avoidant patterns consistently prevent the relationships and life you want—and when self-directed work alone hasn't shifted the cycle. Your avoidant strategies protected you for a long time, and there's no shame in needing support to update them.
Seeking help is itself a counter-avoidant act. The very step that feels hardest—asking another person for support—is already part of the healing.
Specific indicators that therapy would be beneficial:
- You've noticed the same pattern repeating: relationships end because you withdrew when things got close
- Identifying what you're feeling often draws a blank, or you consistently intellectualize emotions instead of experiencing them
- Childhood experiences of neglect, emotional unavailability, or trauma that you haven't processed with a professional
- If close friends or partners have told you that your avoidant patterns are affecting the relationship, that outside perspective matters
- A sense that you want closer relationships but genuinely don't know how to create them
Even severe avoidant presentations can shift through the therapeutic relationship. A case documented in the American Journal of Psychotherapy (2016) showed remission of avoidant personality disorder through earned-secure attachment developed within therapy. The Levy and Johnson (2018) meta-analysis confirmed that therapy produces measurable shifts from insecure to secure attachment on both dimensional and categorical measures.
The Readiness Inventory (for avoidant individuals uncertain about whether they need professional support) Rate each statement from 1 (not true at all) to 5 (completely true):
- I want closer relationships but don't know how to create them
- People have told me I'm emotionally unavailable
- I struggle to name what I'm feeling in the moment
- I've lost relationships because I pulled away
- I feel more stressed than I consciously realize
Score of 15 or higher: therapy is strongly recommended—a therapist trained in attachment can provide the corrective relational experience your nervous system needs. Score of 10 to 14: consider guided self-help combined with app support like Meadow. Score below 10: self-directed work with the exercises in this article may be sufficient for now.
This inventory targets the avoidant tendency to underestimate the need for help. Scoring provides a concrete threshold that bypasses the deactivating strategy of "I can handle this on my own"—because that belief is often the pattern itself.
Frequently Asked Questions
Can avoidant attachment be cured?
Avoidant attachment isn't a disease requiring a "cure"—it's a learned protective pattern that can shift. Research on earned secure attachment shows people move from insecure to secure through self-awareness, therapy, and corrective relational experiences. About 30 percent of adults change attachment style over multi-year periods (Kirkpatrick and Hazan).
How long does it take to heal avoidant attachment?
Research shows attachment shifts occur over months to years, not weeks. Therapy-assisted change can produce measurable differences within 6 to 12 months, while self-directed work through consistent daily practices may take longer. The process is gradual and non-linear—expect progress that looks like a spiral, not a straight line.
What therapy is best for avoidant attachment?
Emotionally Focused Therapy has the strongest evidence for avoidant patterns in couples, with 70 to 75 percent recovery rates (Johnson, 2019). For individuals, CBT augmented with interpersonal and emotional processing outperforms standard CBT alone (Newman et al., 2015). Somatic approaches and Internal Family Systems also show promising results for avoidant individuals who intellectualize in traditional talk therapy.
Can an avoidant person fall in love?
Yes. Avoidant individuals experience love and attachment needs—neuroscience shows these needs exist at an unconscious level even when consciously suppressed (Mikulincer and Shaver). The challenge isn't feeling love but tolerating the vulnerability that closeness brings. Healing involves expanding the capacity for emotional intimacy rather than creating feelings that were never there.
Is avoidant attachment the same as not caring?
No. Avoidant individuals suppress emotional responses through deactivating strategies, but their bodies still show stress responses like elevated cortisol. Research demonstrates a dissociation between reported low distress and physiological arousal—the caring is present but blocked from conscious awareness by a nervous system that learned emotional expression wasn't safe.
Can avoidants become secure without therapy?
Some avoidant individuals shift toward security through consistent secure relationships, self-reflection, and deliberate practice. Research shows trust toward a partner uniquely predicts reduced avoidance over time (Kirkpatrick and Hazan). Therapy significantly accelerates the process, especially for those with unprocessed childhood trauma or difficulty identifying emotions.
What is the difference between dismissive-avoidant and fearful-avoidant?
Dismissive-avoidant individuals suppress attachment needs and maintain emotional distance consistently—they may genuinely believe they don't need close relationships. Fearful-avoidant individuals oscillate between craving closeness and pulling away, experiencing both the desire for connection and the terror of it. Their healing paths differ: dismissive-avoidant focuses on reconnecting with suppressed emotions, while fearful-avoidant focuses on building stability within emotional experiences.
Do avoidants miss you after a breakup?
Research suggests avoidant individuals experience delayed grief because deactivating strategies initially suppress loss-related emotions. The feelings often surface weeks or months later when suppression strategies fatigue. Mikulincer and Shaver's work on deactivating strategies explains this pattern—avoidant individuals can block conscious access to separation-related thoughts, but the unconscious activation of loss and longing persists beneath the surface.
Want to Go Deeper?
Meadow includes a structured assessment to help you understand your specific attachment patterns, followed by a 66-day program of daily practices designed to build earned security.
Start your free week →References
Longitudinal and Prevalence Studies
Roisman, G. I., Padrón, E., Sroufe, L. A., & Egeland, B. (2002). Earned-secure attachment status in retrospect and prospect. Child Development, 73(4), 1204–1219.
Kirkpatrick, L. A., & Hazan, C. Attachment styles and close relationships: A four-year prospective study. Personal Relationships.
Mickelson, K. D., Kessler, R. C., & Shaver, P. R. (1997). Adult attachment in a nationally representative sample. Journal of Personality and Social Psychology, 73(5), 1092–1106.
Chopik, W. J. (2024). Attachment security and how to get it. Social and Personality Psychology Compass.
Therapy Outcome Research
Levy, K. N., & Johnson, B. N. (2018). Attachment and psychotherapy: Implications from empirical research. Canadian Psychology, 60(3). Meta-analysis of 36 studies, N=3,158.
Newman, M. G., Castonguay, L. G., Jacobson, N. C., & Moore, G. A. (2015). Adult attachment as a moderator of treatment outcome for generalized anxiety disorder: Comparison between cognitive-behavioral therapy (CBT) plus interpersonal and emotional processing therapy (I/EP) and CBT plus supportive listening. Journal of Consulting and Clinical Psychology, 83(5), 915–925.
Johnson, S. M. (2019). The practice of emotionally focused couple therapy: Creating connection. Review of EFT outcome research. Couple and Family Psychology: Research and Practice.
Navarro-Gil, M., Lopez-del-Hoyo, Y., Modrego-Alarcón, M., Montero-Marin, J., Van Gordon, W., Shonin, E., & Garcia-Campayo, J. (2018). Effects of attachment-based compassion therapy (ABCT) on self-compassion and attachment style. Mindfulness, 11, 139–153.
Buchheim, A., & Wildmann, A. (2016). Earned-secure attachment: Change of attachment status in treatment and the case of a patient with avoidant personality disorder. American Journal of Psychotherapy, 70(3), 233–250.
Neuroscience
BMC Neuroscience (2021). Attachment avoidance and hippocampal gray matter density. BMC Neuroscience, 22, 617.
DeWall, C. N., Masten, C. L., Powell, C., Combs, D., Schurtz, D. R., & Eisenberger, N. I. (2012). Do neural responses to rejection depend on attachment style? An fMRI study. Social Cognitive and Affective Neuroscience, 7(2), 184–192.
Theoretical Frameworks
Mikulincer, M., & Shaver, P. R. Attachment in adulthood: Structure, dynamics, and change. Deactivating strategies framework.
Porges, S. W. The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation.
Schwartz, R. C. Internal Family Systems therapy. Protector parts framework.
Levine, P. A. Somatic Experiencing: Body-based approaches to trauma resolution.
This article is for educational purposes only and is not a substitute for professional mental health treatment. If avoidant attachment patterns are significantly affecting your relationships or well-being, please consult a licensed therapist who specializes in attachment-based approaches.
